
At the American College of Rheumatology (ACR) Convergence 2025, Dr. Pamela Weiss delivered a focused presentation on the diagnosis and management of axial juvenile spondyloarthritis (axJSpA), highlighting key distinctions and overlaps with adult-onset disease. This targeted article synthesizes the principal objectives and takeaways from that session: identification of the characteristic clinical features of axJSpA, the challenges inherent to imaging the developing sacroiliac joint, the application and limitations of contemporary classification criteria for axial disease in children and current therapeutic strategies for axJSpA.1–4
Juvenile idiopathic arthritis (JIA) is a chronic childhood rheumatic disease affecting approximately 3 per 1,000 children.1 The International League of Associations for Rheumatology (ILAR) classification criteria, currently the most widely used criteria, classify JIA into seven mutually exclusive categories.2,3 Most juvenile spondyloarthritis (JSpA) presentations are captured within the enthesitis-related arthritis (ERA) or juvenile psoriatic arthritis (JPsA) categories, which parallel peripheral and non-radiographic spondyloarthritis (SpA) in adults, respectively.3 Approximately 20% of SpA cases have onset before the age of 18 years, about 20% of children with JIA have JSpA and about 20% of patients with JSpA develop axial disease (axSpA). Axial disease confers substantial morbidity in both pediatric and adult populations.4 This article summarizes the key points from the ACR presentation, briefly elaborates where those are useful and cites relevant literature to contextualize diagnostic and management considerations for axJSpA.
Key features of axial disease in juvenile spondyloarthritis
Compared with adults, children with axJSpA more commonly have concurrent peripheral disease consisting of arthritis and/or enthesitis. Symptoms attributable to axial arthritis are often insidious, worse with rest and improved by movement, while enthesitis pain typically worsens with activity. Extra-articular manifestations, including acute symptomatic anterior uveitis, gut inflammation and psoriasis, can also occur. About 50% of children with JSpA are human leukocyte antigen (HLA)-B27 positive, though it is a lower proportion than in adults.5
Clinical and imaging evidence of axial disease is present at diagnosis in approximately 20% of children and is slightly more frequent in boys.6 On examination, spinal findings, such as limited range of motion or tenderness, may be less pronounced than in adults, and sacroiliac joint tenderness is neither highly sensitive nor specific for sacroiliitis in children. Radiographs are of limited value early in pediatric disease because radiographic changes develop late and can be difficult to interpret; they are therefore often deferred unless required by insurance or to evaluate alternative diagnoses (e.g. stress fracture and infection).7 When axial disease is suspected, a dedicated pelvic magnetic resonance image (MRI) is essential. Pediatric MRI protocols mirror adult practice by not requiring intravenous contrast and, ideally, include T1 and fluid-sensitive coronal oblique sequences; work is ongoing to establish optimized pediatric protocols.
Differences between adult and juvenile onset axial spondyloarthritis
Adult- and juvenile-onset axial SpA share many clinical features, but key distinctions exist. Patients with adult-onset disease are more likely to have a family history of SpA, be HLA-B27 positive and develop acute anterior uveitis. By contrast, patients with juvenile-onset disease more commonly present with peripheral manifestations, including arthritis, hip arthritis and tarsitis, than those with adult-onset disease.8
Challenges of imaging the developing sacroiliac joint
In both adults and children, active sacroiliitis on MRI is defined by subchondral bone marrow edema (BME) on fluid-sensitive sequences. BME may be unilateral or bilateral and is more commonly seen on the iliac side, and associated imaging findings can include sclerosis, fat metaplasia, erosions and ankylosis. Synovitis or joint effusion without BME in children is rare.9
Interpretation of sacroiliac joint MRI in children is challenging and requires familiarity with the normal appearance of the maturing sacroiliac joint, as normal maturational changes can be easily mistaken for pathologic inflammation by the untrained eye (Figure 1).10 During sacral ossification, cartilage apophyses and newly formed bone produce high signal on fluid-sensitive sequences.11,12 This signal typically disappears as apophyses fuse with skeletal maturity. These maturational changes are usually bilateral and symmetric, following the contours of the sacral apophyses.13 Published atlases describing MRI inflammatory and structural lesions typical of JSpA have been published and may help less experienced providers distinguish physiologic maturation from true pathology.11,14
Figure 1: Normal maturational signal in youth along the sacroiliac joints
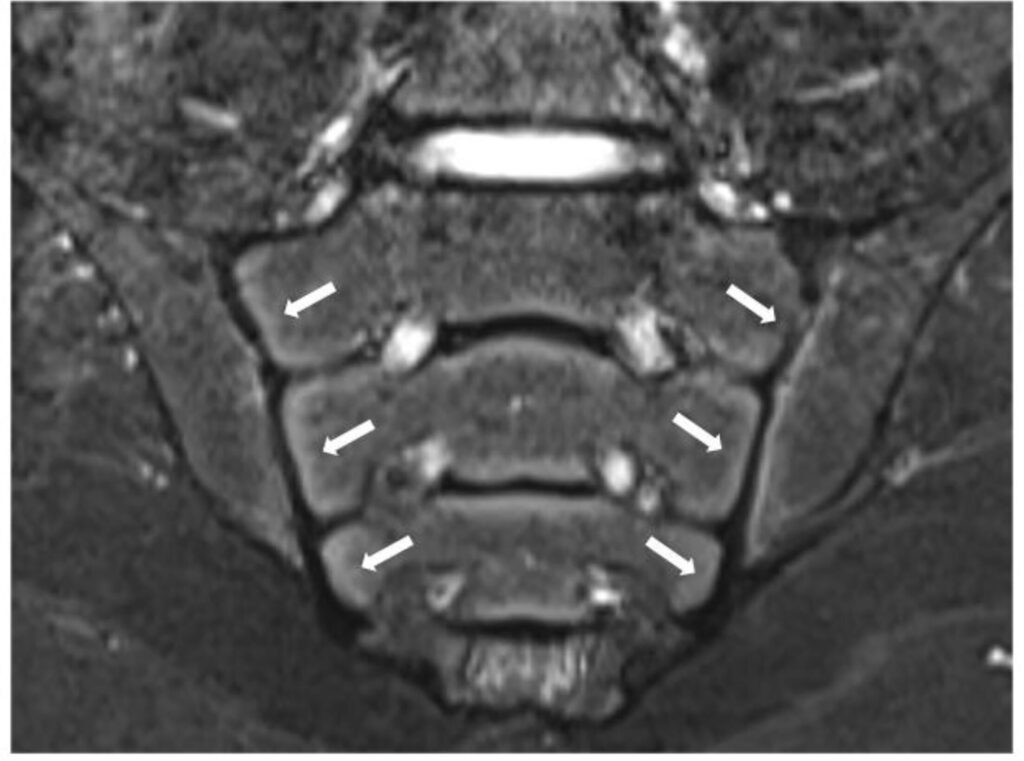
Sacroiliac joints of a an 8-year-old male patient are shown. Short tau inversion recovery (STIR) fluid sensitive coronal oblique image of the pelvis demonstrates symmetric, maturational high signal along the sacral apophyses (arrows). These findings reflect normal ossification and cartilage apophyses in a skeletally immature child and should not be mistaken for inflammatory bone marrow edema
Current pediatric classification criteria for axial disease
Although axial symptoms (sacroiliac tenderness or inflammatory back pain) are included in the ILAR definition of ERA, they are neither sensitive nor specific; about one-quarter of children with axial disease do not fulfill the criteria for ERA or any ILAR JIA category.15 To improve the identification of JSpA with axial involvement and support trials in this population, specific classification criteria for axial JSpA (axJSpA) were developed and validated.16 These criteria were derived through a four-phase process: item generation, item reduction, criteria development and validation. The final criteria incorporate domains for imaging of active inflammation, imaging of structural lesions, chronicity of pain, pain pattern and location, stiffness and genetics. Scores range up to 100, with ≥55 required for classification (Table 1), and online scoring tools are available (https://redcap.link/axjspa_cc).16 The axJSpA criteria apply to patients with pediatric disease with a clinical diagnosis of JSpA and suspected axial disease and proved more sensitive and specific for youth than the adult Assessment of SpondyloArthritis International Society (ASAS) non-radiographic axSpA criteria.17
Table 1: Axial juvenile spondyloarthritis classification criteria16
| Criteria level | Domains | Weight | Maximum domain score |
| Imaging: active inflammation | |||
| 0 | No unequivocal evidence of active lesions typical of sacroiliitis on MRI | 0 | 23 |
| 1 | Unequivocal evidence of active lesions typical of sacroiliitis on MRI | 23 | |
| Imaging: structural lesions | |||
| 0 | No unequivocal evidence of structural lesions typical of sacroiliitis on MRI | 0 | 23 |
| 1 | Unequivocal evidence of sacroiliitis on radiograph | 13 | |
| 2 | Unequivocal evidence of structural lesions typical of sacroiliitis on MRI | 23 | |
| Pain chronicity | |||
| 0 | No pain or pain <4 days per week or for <6 weeks | 0 | 9 |
| 1 | Most days (>4 days per week) for >6 but<12 weeks | 6 | |
| 2 | Most days (>4 days per week) for >12 weeks | 9 | |
| Pain pattern | |||
| 0 | No identifiable pain pattern | 0 | 13 |
| 1 | Awakens patient in the second half of the night or insidious onset | 6 | |
| 2 | Moderate to total relief with NSAIDs | 10 | |
| 3 | Improves with activity | 13 | |
| Pain location | |||
| 0 | No back, groin, hip or buttock pain | 0 | 12 |
| 1 | Lumbar spine pain (patient-reported symptom) | 6 | |
| 2 | Sacroiliac pain with deep palpation/provocation maneuver(s) or groin/hip pain (patient-reported symptom) | 11 | |
| 3 | Sacral/buttock pain (patient-reported symptom) | 12 | |
| Stiffness (morning) | |||
| 0 | Stiffness <15 min | 0 | 9 |
| 1 | Stiffness for ≥15 min | 9 | |
| Genetics | |||
| 0 | No relevant family history in first-degree relative and/or HLA-B27 unknown or negative | 0 | 11 |
| 1 | Presence of the following in a first-degree relative: SpA or HLA-B27-associated acute anterior uveitis | 8 | |
| 2 | Presence of HLA-B27 | 11 | |
Table lists the domains, levels and weights for the axJSpA classification criteria. The far right column lists the maximum score per domain. Levels within each domain are mutually exclusive, and the highest level achieved within each domain contributes to the overall score. Maximum score is 100, and scores of 55 and above meet the threshold for classification as AxJSpA
HLA-B27 = human leukocyte antigen B27; MRI = magnetic resonance image; NA = not applicable; NSAIDs = nonsteroidal anti-inflammatory drugs; SpA = spondyloarthritis.
There are several key differences between the AxJSpA criteria and the adult ASAS AxSpA criteria. For the AxJSpA criteria, children must have a clinical diagnosis of JSpA, suspected axial disease and an age of onset of less than 18 years. For the adult ASAS non-radiographic axSpA criteria, the patient must have had back pain for at least 3 months and must be less than 45 years of age at symptom onset. In contrast to the adult criteria, which require back pain, the axJSpA criteria include pain localized to the hips, groin or back that may be present for as few as 6 weeks. Unlike the adult criteria, which can be met by either the clinical or imaging arm, the axJSpA criteria require both imaging evidence of sacroiliitis (inflammatory and/or structural) and compatible clinical symptoms to exceed the threshold.16,18 These pediatric criteria are intended to enable rigorous clinical trials, advance drug evaluation and approval, and improve understanding of axJSpA.
Treatment algorithms and therapeutic approaches for pediatric axial spondyloarthritis
Treatment of children with JSpA is guided primarily by the extent of peripheral joint involvement and the presence of sacroiliitis. The ACR Guideline 2019 for the treatment of JIA and sacroiliitis strongly recommends a nonsteroidal anti-inflammatory drug (NSAID) over no NSAID and advises adding a tumor necrosis factor inhibitor (TNFi) when sacroiliitis remains active despite an adequate trial of NSAIDs.19 The guideline also strongly discourages methotrexate monotherapy for sacroiliitis. Beyond TNFi therapy, there are no pediatric-specific guidelines for treating axJSpA. Although secukinumab (an IL-17 inhibitor) is approved for children with ERA, data on its efficacy in pediatric axial disease are lacking, and it is not yet included in treatment guidelines. Similarly, evidence for Janus Kinase-Signal Transducer and Activator of Transcription inhibitors and other therapeutic classes in pediatric axial SpA is very limited to date.
When treated with TNFi therapy, most children with axial SpA show clinically meaningful improvements in pain and function by 3 months.20 Although routine follow-up imaging after TNFi initiation is not standard clinical practice, research protocols have demonstrated objective imaging improvements by 3 months, with further gains by 6 months.20
Disease course and long-term trajectory of pediatric axial spondyloarthritis
Studies directly comparing outcomes between juvenile- and adult-onset axial disease are limited. This gap likely reflects, at least in part, the historical lack of standardized classification criteria for juvenile-onset axial disease (other than ankylosing spondylitis, which represents a more advanced stage). Until the recent development and validation of the axJSpA criteria, it was difficult to assemble comparable cohorts of youth and adults for meaningful comparisons of outcomes. In a 2009 cross-sectional study by Gensler et al., functional outcomes did not differ significantly between juvenile- and adult-onset ankylosing spondylitis.21 However, spinal radiographic severity, measured by the Bath Ankylosing Spondylitis Radiology Index (BASRI), was significantly greater in the adult-onset group across the total spine, as well as the lumbar and cervical regions. By contrast, BASRI scores for the hip were significantly worse in those with juvenile-onset disease.
Conclusion
In summary, axJSpA, which begins before the age of 18 years in approximately 20% of cases, has been difficult to study until now because of the absence of classification criteria. The recently validated axJSpA criteria with online scoring tools should enable more rigorous research. Compared with adults, youth more often have peripheral and root-joint disease and less acute uveitis, with similar functional outcomes but greater hip and less spinal radiographic involvement. MRI of the sacroiliac joint can be challenging and requires familiarity with the appearance of maturational changes. Treatment data remain limited: most patients respond to TNF inhibitors, secukinumab is approved for ERA but not yet established for pediatric axial disease and no therapies are FDA-approved specifically for axJSpA. The new criteria provide an important foundation for advancing clinical trials and optimizing care for affected children.



