
Autoimmune rheumatic diseases (AIRDs) predominantly affect women during their reproductive years and are associated with increased risks of infertility and adverse pregnancy outcomes (APOs). These diseases, such as systemic lupus erythematosus (SLE), antiphospholipid antibody syndrome (APS) and rheumatoid arthritis (RA), carry a substantial risk of pre-eclampsia (PEC), recurrent miscarriages, preterm birth (PTB) and foetal growth restriction (FGR).1 Over the past two decades, however, advances in preconception risk stratification, the availability of pregnancy-safe immunomodulatory therapies and multidisciplinary care models have markedly improved pregnancy outcomes, enabling many women with AIRDs to pursue pregnancy and positioning reproductive healthcare as a core domain of contemporary rheumatology practice.2
A large population-based registry highlights the on-going reproductive burden of AIRDs.3 A Finnish registry of 5.3 million individuals demonstrated higher rates of childlessness among women with AIRDs compared with matched controls (≈3.6% overall), with the greatest disparity observed in juvenile idiopathic arthritis (JIA), where lifetime childlessness approached 9%.3 Pregnancy-related risk is particularly pronounced in systemic sclerosis (SSc); in a prospective cohort of high-risk pregnancies, women with SSc experienced significantly higher composite APOs than those with SLE and healthy controls, driven by miscarriage, PEC, PTB and small-for-gestational-age infants.4 These data underscore that AIRDs impose a multisystem burden and impact fertility and pregnancy outcomes.
This paradigm shift integrates proactive care of reproductive health into routine rheumatology, with the updated European Alliance of Associations for Rheumatology (EULAR) 2024 guidelines and American College of Rheumatology (ACR) 2020 guidelines advocating early family-planning discussions and preconception counselling as standard components of management of AIRDs.5,6 Nevertheless, implementation remains inconsistent, with delayed or suboptimal counselling regarding contraception, fertility preservation and pregnancy planning contributing to the critical care gap.7 This gap has important clinical consequences, as uncontrolled disease activity, teratogenic medications and pathogenic autoantibodies (e.g. anti–Sjögren’s-syndrome-related antigen A [anti-Ro/SSA], antiphospholipid antibodies [aPL]) substantially influence maternal and foetal outcomes. Addressing these challenges requires coordinated multidisciplinary care involving rheumatology, maternal–foetal medicine, nephrology, cardiology and endocrinology. The benefits of such integration are evident in reproductive rheumatology clinics; the UK joint rheumatology–obstetric service reported a 97% live-birth rate across 98 AIRD pregnancies, with gestational age and birth weights comparable to the general population.8
Effective management of pregnancy in AIRDs requires understanding trimester-specific immunological adaptations that support foetal tolerance. Immune dysregulation and disease-specific autoantibodies can disrupt these processes, resulting in APOs. This convergence of immunology, reproductive medicine and rheumatology has given rise to the concept of ‘reproductive rheumatology’ – a growing subspecialty focusing on reproductive health across the AIRDs. First articulated by Dr Eliza Chakravarty, this framework reflects the evolving recognition that successful outcomes in AIRDs now extend beyond survival to informed family planning, healthy pregnancy and long-term reproductive wellbeing.9
Emergence and scope of reproductive rheumatology
Reproductive rheumatology has emerged as a distinct clinical focus within rheumatology, addressing reproductive health across the life course in individuals with AIRDs, including family planning, fertility, pregnancy, postpartum care, lactation and menopause.6 Male patients with inflammatory arthritis may also benefit from structured reproductive health counselling.10 This integrated framework is reflected in major guidelines, such as ACR 2020, which comprehensively addresses contraception, fertility preservation, pregnancy, lactation and menopausal hormone therapy in individuals with AIRDs.6 The updated EULAR recommendations reinforce the central role of sustained disease control during pregnancy, endorsing pregnancy-compatible therapies such as hydroxychloroquine (HCQ), while advising against the use of established teratogens, including methotrexate (MTX).5 While inherently multidisciplinary, this subspecialty centres on the rheumatologist’s role in integrating immunological and pharmacological expertise into individualized reproductive planning.
The relevance of reproductive rheumatology is underscored by the female predominance and reproductive-age onset of many AIRDs, including SLE, RA, SSc, etc., underscoring a need for prospective dedicated registries.11 Data from the prospective Italian Pregnancy in Rheumatic Diseases (P-RHEUM.it) registry (866 pregnancies) demonstrate the broad diagnostic spectrum of AIRDs, including inflammatory arthritides, connective tissue diseases and systemic vasculitides, with SLE being the most frequent diagnosis (19.6%).12 These findings highlight the need for expert, coordinated care across diverse AIRDs.
Reproductive rheumatology is increasingly recognized as a continuous, lifecycle-based model rather than being limited to pregnancy-related interventions.6,13 Clinical priorities evolve across preconception, pregnancy, postpartum, lactation and contraception, each phase presenting distinct immunological, pharmacological and psychosocial considerations. Importantly, this continuum extends beyond the reproductive years into the menopausal transition and later life, as women with AIRDs experience accelerated reproductive ageing driven by chronic inflammation and cumulative gonadotoxic exposure, with important implications for bone, cardiovascular, metabolic and psychosocial health.13 In line with this, the 2020 ACR reproductive health guidelines advocate a lifespan-based approach encompassing contraception, fertility preservation, pregnancy, lactation and menopausal hormone therapy, emphasizing anticipatory counselling and individualized management across all reproductive stages, including menopause, to optimize long-term outcomes.6 This lifecycle-based framework and its stage-specific clinical priorities are illustrated in Figure 1, with key definitions and core concepts summarized in Table 1.5,12
Figure 1: Reproductive lifecycle in autoimmune rheumatic diseases
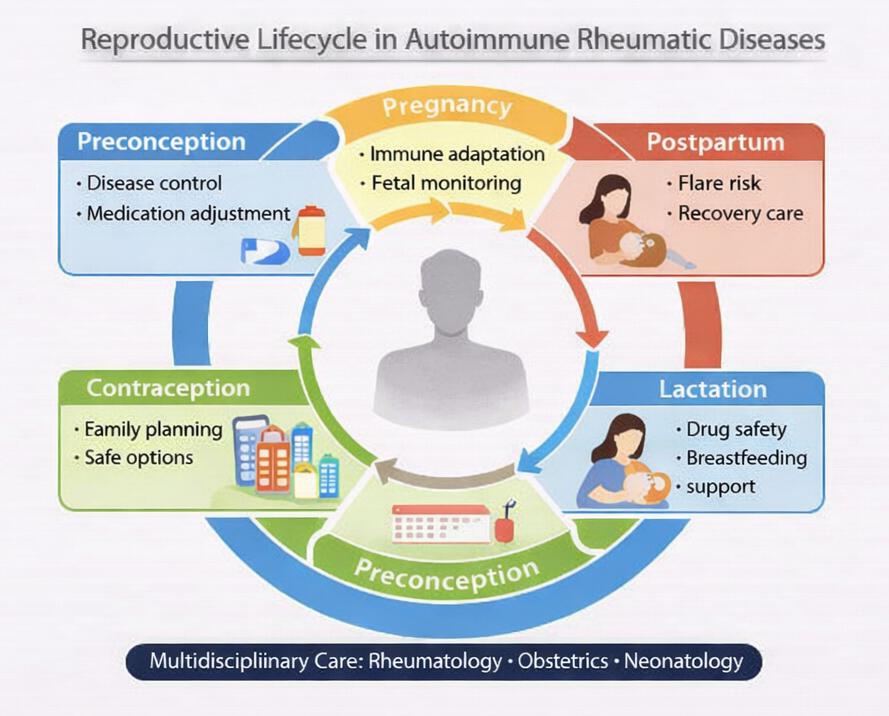
Figure 1 was recreated programmatically using Python 3.13 and Matplotlib 3.10.8.
Table 1: Key definitions and concepts in reproductive rheumatology5,12
| Clinical pillar | Term | Scientific definition and clinical context |
| Integrated care | Reproductive rheumatology5,12 | The specialized, integrated management of fertility, pregnancy, postpartum and lactation specific to patients with AIRDs |
| Strategy | Preconception counselling5,12 | Comprehensive risk stratification and medication optimization to ensure disease stability before attempting conception and to reduce preventable maternal–foetal complications |
| Risk mitigation | Teratogenic drugs5,12 | Agents strictly contraindicated due to established foetal risk (MTX, MMF, CYC); these must be discontinued during the pregnancy-planning phase with appropriate washout periods where applicable |
| Optimization | T2T5 | A protocol of achieving and maintaining remission or low disease activity using pregnancy-compatible therapies, with proactive monitoring and timely treatment adjustments |
| Vigilance | Disease flare5,12 | A clinically significant increase in inflammatory disease activity requiring escalation or adjustment of therapy, often involving multidisciplinary review to balance maternal control and foetal safety |
| Recovery | Postpartum relapse5 | A flare occurring after delivery, typically driven by rapid immunological and hormonal rebound, requires anticipatory planning, close monitoring and early treatment optimization |
| Continuity | Lactation-compatible therapy5 | Medications considered safe during breastfeeding, enabling sustained maternal disease control while supporting lactation goals and minimizing infant drug exposure |
AIRDs = autoimmune rheumatic diseases; CYC = cyclophosphamide; MMF = mycophenolate mofetil; MTX = methotrexate; T2T = treat-to-target.
This framework emphasizes the dynamic nature of disease activity and immunological shifts across reproductive stages and highlights the importance of integrated multidisciplinary care involving rheumatology, obstetrics/maternal–foetal medicine and neonatology (Figure 1).
Key diseases and demographic drivers of reproductive rheumatology
Reproductive rheumatology spans the full spectrum of individuals with AIRDs of reproductive age, reflecting both disease-specific risks and their demographic distribution.12 Conditions such as SLE and APS require meticulous pregnancy planning, including assessment of disease activity, achievement of disease remission, evaluation of pathogenic autoantibodies and individualized treatment to mitigate maternal and foetal risk.5,6 In RA, psoriatic arthritis (PsA) and spondyloarthritis (SpA), management frequently necessitates modification of disease-modifying therapy, including discontinuation of teratogenic agents, alongside close monitoring of disease activity throughout pregnancy.5,6 Other AIRDs, including SSc, inflammatory myopathies, systemic vasculitides and JIA, pose additional challenges related to organ involvement (e.g. pulmonary hypertension or renal and cardiac disease) and may warrant consideration of fertility preservation.2,4,6
These disease-specific complexities are amplified by the epidemiology of AIRDs, which disproportionately affect women during their reproductive years. Many AIRDs demonstrate a marked female predominance, particularly SLE and SSc, with female-to-male ratios approaching 9:1 and approximately 78% of affected individuals being women.13–15 Disease onset most commonly occurs between late adolescence and the fourth decade of life.16 RA affects approximately 1% of the population and predominantly women, with typical onset between the mid-20s and early 50s, while SLE frequently presents in young women from late adolescence through the 30s.17 Population-based data from the UK further illustrate the growing relevance of reproductive health in AIRDs, with the prevalence of AIRDs among pregnant women increasing from approximately 3.5% in 2000 to 4.7% in 2021, representing an absolute rise of about 1.2% and a relative increase of nearly one-third.18
Collectively, these epidemiological and disease-specific factors underscore the necessity for individualized, multidisciplinary reproductive care guided by international recommendations and real-world registry evidence across all AIRDs.5,6,12,17,18
Impact of disease on reproductive outcomes
Many women with AIRDs experience challenges with fertility. RA and SpA are associated with prolonged time-to-pregnancy, being >12 months in 32–42% of cases, potentially due to reduced ovarian reserve, chronic inflammation and periconceptional exposure to medicines such as non-steroidal anti-inflammatory drugs (NSAIDs).19,20
Even when conception is achieved, APOs such as miscarriage, PTB, PEC, FGR and low birth weight are increased in SLE, APS, RA and other AIRDs.21,22 A recent systematic review and meta-analysis of 72 studies, including 10,355 pregnancies in SLE, identified key predictors of APOs.23 Prior lupus nephritis or pre-existing chronic hypertension significantly increased the risk of overall APOs (odds ratio [OR]: 2.00; 95% confidence interval [CI]: 1.55–2.57; I²=17%) and PEC (OR: 3.11; 95% CI: 2.35–4.12; I²=0%).23 Comparative data from a multicentre cohort of 189 pregnancies demonstrated more favourable outcomes in SpA than in RA or PsA, with higher live birth rates (89.7% versus 76.3%) and lower miscarriage rates (10% versus 21% and 31%, respectively).24 PTB remains common across several AIRDs, reported in approximately 20–40% of SLE, 24–60% of SSc, 30–50% of APS and 16–20% of RA pregnancies, while rates are consistently lower in PsA and SpA (≈6–10%). In the same cohort, PTB occurred in 16% of RA pregnancies compared with 6.9% in PsA.24 Given the heterogeneity in obstetric and maternal risk profiles across AIRDs, a disease-specific overview of key pregnancy complications is summarized in Table 2.
Table 2: Disease-specific reproductive considerations and pregnancy risks in women across major autoimmune rheumatic diseases
| AIRD | Preconception | Conception Major risks and monitoring focus | Postpartum Key considerations |
| SLE | Achieve sustained remission/low activity (≥6 months prior to pregnancy planning); evaluate nephritis activity; screen autoantibodies (aPL, anti-Ro/La); optimize pregnancy-compatible therapy | Disease flares, monitor blood pressure for pre-eclampsia evidence, foetal growth restriction, preterm birth, urine protein, complement levels/anti-dsDNA; foetal heart surveillance when anti-Ro/La positive | High flare risk; early re-escalation of therapy if flare; thrombosis prevention where indicated; ensure breastfeeding-compatible regimen |
| APS | Thrombosis and obstetric risk stratification, confirm persistent aPL positivity; plan antithrombotic strategy | Pregnancy loss, placental insufficiency, pre-eclampsia, foetal growth restriction, thrombosis; close maternal–foetal monitoring | Continue anticoagulation postpartum when indicated; heightened vigilance for thromboembolism; coordinate with obstetrics/medicine |
| RA | Transition from teratogenic agents to compatible DMARDs; ensure stable disease before conception | Many patients improve or remain stable; however, active disease may still occur; monitor functional limitation and analgesic needs | Frequent postpartum flares: early restart/optimize effective therapy compatible with lactation |
| SpA | Control axial/peripheral disease; review NSAIDs and biologic plan; assess mobility and functional status | Variable course: pain control and functional limitation may persist; monitor disease activity and need for pregnancy-compatible biologics | Flare risk postpartum; plan breastfeeding-compatible DMARD strategy; physiotherapy and rehabilitation support |
| Systemic vasculitis | Aim for remission or stable low disease activity prior to conception; assess baseline organ damage (renal, pulmonary, cardiac); optimize immunosuppression plan | Relapse risk, hypertension, foetal growth restriction, prematurity; careful monitoring of organ function and medication safety | Postpartum relapse possible; immunosuppression adjustment; monitor blood pressure/renal function; infection risk counselling |
| Systemic sclerosis | Assess pulmonary hypertension/interstitial lung disease, renal status, cardiac involvement; optimize blood pressure control; counsel high-risk pregnancy if advanced disease | Increased risk of hypertensive disorders, foetal growth restriction, prematurity; monitor blood pressure, renal function, cardiopulmonary status; vigilance for scleroderma renal crisis | Monitor for blood pressure instability/renal complications; adjust immunosuppression cautiously; multidisciplinary follow-up essential |
| Sjögren’s Disease | Screen anti-Ro/SSA and anti-La/SSB; counsel foetal surveillance plan; optimize compatible therapy | Risk of neonatal lupus and congenital heart block (anti-Ro/La positive); foetal echocardiographic monitoring where appropriate; maternal fatigue and systemic activity monitoring | Postpartum disease activity monitoring; maintain breastfeeding-compatible treatment; counselling on neonatal follow-up if exposed risk present |
AIRD = autoimmune rheumatic disease; anti-dsDNA = anti–double-stranded DNA antibodies; anti-La/SSB = anti–Sjögren’s-syndrome-related antigen B antibodies; anti-Ro/SSA = anti–Sjögren’s-syndrome-related antigen A antibodies; aPL = antiphospholipid antibodies; APS = antiphospholipid syndrome; DMARDs = disease-modifying antirheumatic drugs; NSAIDs = non-steroidal anti-inflammatory drugs; RA = rheumatoid arthritis; SLE = systemic lupus erythematosus; SpA = spondyloarthritis.
Disease quiescence at conception is associated with improved pregnancy outcomes in AIRDs; in the P-RHEUM.it prospective registry, 91.7% of pregnancies resulted in live births on pregnancy-compatible treatment strategies.12,25 Cumulatively, these realities of gender bias, childbearing age onset and elevated pregnancy risks warrant a dedicated focus on reproductive care in rheumatology.
Medication considerations
A key challenge in reproductive rheumatology is balancing optimal maternal disease control against potential foetal risk. While disease activity itself is a major determinant of APOs, many conventional and biologic disease-modifying antirheumatic drugs (DMARDs) have limited data on pregnancy safety, complicating treatment decisions.25 Established teratogens, including MTX, mycophenolate mofetil (MMF) and cyclophosphamide (CYC), must be discontinued well in advance of conception, but both CYC and MMF may be considered in selected severe organ- or life-threatening disease during the second and third trimesters.5,26–28
Conversely, several immunomodulatory therapies have now been shown to have reassuring safety profiles across pregnancy and lactation, allowing continuation when clinically indicated to maintain disease control.5,26,27 These advances have shifted clinical practice away from blanket drug withdrawal towards individualized, risk-adapted treatment strategies. Tumour necrosis factor inhibitors (TNFis), in particular, are increasingly regarded as relatively low risk during pregnancy, with agent- and timing-specific considerations.5,6,26 In contrast, newer targeted therapies, including Janus kinase inhibitors and selected monoclonal antibodies, remain limited by sparse human pregnancy data, necessitating a precautionary approach.5,6,27
Medication planning around conception, therefore, requires proactive, evidence-based counselling, timely discontinuation of teratogenic agents and selection of therapies with established reproductive safety profiles.5,6,27,29 Table 3 summarizes the compatibility of commonly used antirheumatic drugs across preconception, pregnancy, postpartum and lactation, based on the updated EULAR 2024 and the ACR 2020 guidelines.5,6
Table 3: Safety/compatibility of common antirheumatic drugs across reproductive stages in AIRDs based on ACR 2020 and updated EULAR 2024 guidelines5,6
| Drug (class) | Preconception | First trimester | Second–third trimester | Postpartum | Lactation |
| Hydroxychloroquine | Compatible (continue) | Compatible | Compatible | Compatible | Compatible |
| Sulfasalazine (+ folic acid) | Compatible | Compatible | Compatible | Compatible | Compatible |
| Azathioprine | Compatible | Compatible | Compatible | Compatible | Compatible |
| Tacrolimus (CNI) | Compatible (selected indications, e.g. SLE nephritis) | Compatible | Compatible | Compatible | Compatible |
| Cyclosporine (CNI) | Compatible (selected indications) | Compatible | Compatible | Compatible | Compatible |
| Colchicine | Compatible (where indicated) | Compatible | Compatible | Compatible | Compatible/likely acceptable* |
| Prednisolone (low dose) | Compatible | Caution: lowest effective dose | Caution: lowest effective dose | Compatible | Compatible (timing advice if higher dose) |
| NSAIDs (e.g. ibuprofen/naproxen) | Compatible (short courses) | Caution: lowest dose/short duration | Caution: avoid in late T3 (ductal constriction/oligohydramnios risk) | Compatible | Compatible (short courses) |
| TNFis | Compatible | Compatible | Caution: agent/timing-specific (placental transfer increases later gestation) | Compatible | Compatible |
| Rituximab (anti-CD20) | Caution: consider timing; reserve for severe disease where needed | Restricted: severe/organ-threatening disease only | Restricted: late exposure may affect neonatal B cells | Compatible if required | Compatible (ACR permits; EULAR generally specialist case) |
| IL-6 inhibitors (e.g. tocilizumab) | Caution/avoid preferred switch pre-pregnancy if possible | Avoid unless no alternatives | Avoid unless no alternatives | Avoid unless compelling | Caution (limited data) |
| IL-17 inhibitors (e.g. secukinumab/ixekizumab) | Consider if needed for maternal disease control | Consider if needed for maternal disease control | Consider if needed for maternal disease control | Consider if needed for maternal disease control | Can be considered |
| Methotrexate | Contraindicated (stop ≥3 months) | Contraindicated | Contraindicated | Avoid | Avoid |
| Mycophenolate mofetil | Contraindicated (stop ≥6 weeks) | Contraindicated | May be considered in severe organ or life-threatening disease | Avoid | Avoid |
| Leflunomide | Contraindicated (washout required) | Contraindicated | Contraindicated | Avoid | Avoid |
| Cyclophosphamide | Avoid (reserve for life-threatening disease) | Restricted: life-threatening only | May be considered in severe organ or life-threatening disease | Avoid | Avoid |
| JAK inhibitors | Avoid/contraindicated | Contraindicated | Contraindicated | Avoid | Avoid |
| Antirheumatic drugs in male patients | Azathioprine, colchicine, cyclosporine, hydroxychloroquine, leflunomide, methotrexate ≤25 mg/week, mycophenolate, NSAIDs, prednisone, sulfasalazine, tacrolimus, TNFi bDMARDs and non-TNFi bDMARDs can be continued in male patients trying to conceive Cyclophosphamide: dose-dependent irreversible infertility risk; fertility preservation advised | ||||
Compatible = generally acceptable when clinically indicated.
Caution = timing/dose/agent-specific; specialist monitoring.
Avoid/contraindicated = not recommended (teratogenicity/toxicity/insufficient safety).
*Limited data; considered compatible with breastfeeding based on available evidence.
ACR = American College of Rheumatology; bDMARDs = biologic disease-modifying antirheumatic drugs; CD20 = cluster of differentiation 20; CNI = Calcineurin inhibitor; EULAR = European Alliance of Associations for Rheumatology; IL = interleukin; JAK = Janus kinase; NSAIDs = non-steroidal anti-inflammatory drugs; SLE = systemic lupus erythematosus; T3 = third trimester; TNFis = tumour necrosis factor inhibitors.
Key challenges in reproductive rheumatology
Disease-related challenges
Disease activity of AIRDs increases APOs, with flares rates and patterns varying across different AIRDs, SLE (25–50% during pregnancy; 25–30% postpartum), RA (15–40% during pregnancy; 40–50% postpartum), SpA/PsA (up to 55–90% postpartum) and SSc (15–25% overall).30–32 Even with optimized care, one cohort reported flares in 24% of pregnancies in patients with SLE.31 Preconception disease activity in SLE strongly predicts APOs, with active disease elevating risks of flares, nephritis, PTB (2·00 [1·55–2·57]; I2=17%) and PEC (3·11 [2·35–4·12]; I2=0%).31 Organ-threatening manifestations, including lupus nephritis, pulmonary hypertension or vasculitis in SLE, pulmonary fibrosis in SSc and anti-neutrophil cytoplasmic antibodies (ANCA)-associated glomerulonephritis, substantially raise maternal morbidity, while venous thromboembolism risk is increased 5–20-fold in APS.2,17,33 Overall, active or severe organ involvement markedly heightens obstetric risk across AIRDs.21,33
Pregnancy-related immunological adaptations help explain the distinct flare patterns observed across AIRDs.34,35 Early gestation is associated with a relative shift towards pro-inflammatory immune responses, which may contribute to disease flares in SLE, while RA often shows clinical improvement during pregnancy. As gestation progresses, a regulatory T-cell-dominant, tolerance-promoting immune milieu may contribute to improvement in some AIRDs such as RA, whereas SLE activity may persist due to on-going autoantibody-driven immune dysregulation.34,35 Following delivery, loss of pregnancy-associated immune tolerance and a rebound towards pro-inflammatory immunity are associated with increased postpartum disease activity.34,35
These immunological effects interact with disease-specific risk factors. For example, a recent meta-analysis demonstrated that chronic hypertension in SLE, which often reflects underlying renal or vascular involvement, was associated with a twofold increase in PTB and more than a fivefold increase in the risk of PEC.23 In addition, PEC increases future cardiovascular disease risk, driven by endothelial dysfunction, immune-mediated vascular injury, systemic inflammation and placental malperfusion, leading to persistent vascular remodelling, arterial stiffness and accelerated atherosclerosis.36,37 Beyond obstetric outcomes, underexplored domains include mental health, quality of life (QoL), postpartum depression and emotional distress.38,39 Postpartum flares and depression are common across conditions such as RA, PsA and axial SpA, while many of the AIRDs are also associated with significant sexual dysfunction (SD) in both men and women.40 These issues, including psychological morbidity and SD, adversely affect disease outcomes, maternal wellbeing, couple intimacy and QoL, highlighting the need for integrated physical, psychological and reproductive healthcare in this population.38–40
Together, these factors illustrate the central therapeutic dilemma in reproductive rheumatology: active disease poses substantial risks to both mother and foetus, yet treatment options must be carefully balanced against potential foetal harm.5,6
Healthcare system–related challenges
Limited pregnancy safety data for many drugs in individuals with AIRDs management continue to complicate the selection of treatment and its timing in patients in the reproductive-age group.41 Current guidelines are therefore frequently conditional and consensus-driven, reflecting robust data for some agents and substantial uncertainty for others.5,6,28 Accordingly, reproductive health guidelines from the ACR, EULAR and British Society for Rheumatology (BSR) consistently emphasize the low certainty of evidence or expert consensus underpinning many recommendations for medicines during pregnancy and lactation.5,6,28 While established teratogens are clearly contraindicated, on-going uncertainty persists for newer targeted therapies and for treatment decisions in the postpartum period. Additional concerns, such as infant vaccination following in utero biologic exposure, have been partially mitigated by reassuring registry data for TNFi, whereas evidence for newer agents remains limited.5,42 Paternal drug exposure adds further complexity, although available large-scale observational data do not suggest a significant increase in APOs with commonly used DMARDs.27
Reproductive care for women with AIRDs remains fragmented, with counselling and management often dispersed across multiple specialties. Though structured, rheumatology-led multidisciplinary pregnancy services improve care coordination, counselling consistency and continuity, such models remain inconsistently implemented due to health-system resource constraints.43,44 Documentation of reproductive health counselling is particularly poor; in the US Rheumatology Informatics System for Effectiveness (RISE) registry, contraception and family-planning documentation rates were below 10%, and similarly low rates exist in the UK, with disproportionately lower documentation among minority populations.45,46 These gaps are further amplified in low-resource settings, where limited access to biologics, advanced obstetric imaging and neonatal lupus screening restricts care, and postpartum flares reported in up to 20–50% of cases are often inadequately monitored or managed.12,47 Collectively, these challenges underscore the need for scalable solutions such as rheumatology-led pregnancy clinics, electronic medical record (EMR)–based counselling prompts and targeted clinician training to support individualized, evidence-informed decisions and ensure equitable reproductive care for women with AIRDs.43,44,48
Patient-centred challenges
From the patient’s perspective, reproductive health in AIRDs is burdened by intense fear that pregnancy may trigger flares, harm the foetus or transmit autoimmunity, leading to ambivalence about childbearing, stigma and decisional conflict.43 Uncertainty about the safety of DMARDs during pregnancy and breastfeeding further contributes to the challenges.44 Mental health needs are also substantial, with a large Danish cohort study finding postpartum psychiatric disorders in 1.8% of women with RA versus 1.1% without (adjusted hazard ratio [HR] about 1.4), and a bidirectional link between postpartum depression and other perinatal mood disorders and AIRDs.39 Misinformation and discordant advice between rheumatology, obstetric and primary-care teams are common, while recent surveys of rheumatologists highlight gaps in training, limited use of standardized pregnancy-intention screening and scarce patient-friendly resources.7,46
Potential solutions and evolving models
Preconception counselling and risk stratification
Preconception counselling is a crucial aspect of reproductive rheumatology, comprising routine reproductive counselling for all women of childbearing potential with AIRDs, planned conception during disease remission or low activity on pregnancy-compatible therapy, and comprehensive pre-pregnancy assessment of disease activity and cumulative organ damage, targeted laboratory testing, appropriate imaging, vaccination status and managing relevant comorbidities such as hypertension and diabetes.5,6,49,50 Women with high-risk features, including lupus nephritis, APS or pulmonary arterial hypertension, should be referred early to maternal–foetal medicine or specialized multidisciplinary centres.5,6,51 A potential clinical work flow integrating reproductive goal assessment, treat-to-target disease control, medication optimization and coordinated monitoring is illustrated in Figure 2.
Figure 2: Clinical work flow for reproductive goal assessment and pregnancy planning in autoimmune rheumatic diseases
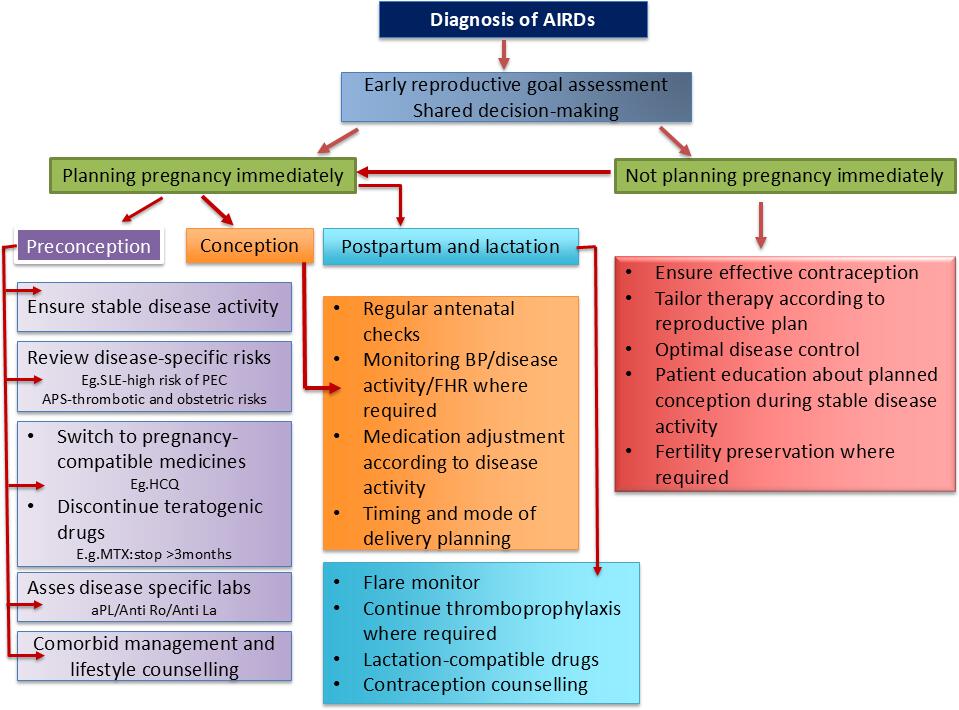
Figure 2 was created using Microsoft PowerPoint (Redmond, WA, USA)
AIRD = autoimmune rheumatic diseases; aPL = antiphospholipid antibodies; APS = antiphospholipid syndrome; BP = blood pressure; FHR = fetal heart rate; HCQ = hydroxychloroquine; La = La antigen (anti-La antibody); MTX = methotrexate; PEC = pre-eclampsia; Ro = Ro antigen (anti-Ro antibody); SLE = systemic lupus erythematosus
Beyond medication review, preconception counselling enables disease-specific risk stratification, identifying predictors of APOs, including active nephritis, high disease activity in SLE, pulmonary hypertension in SSc or SLE, ANCA-associated renal disease in vasculitis, reduced ovarian reserve in inflammatory arthritis and advancing maternal age.6 In SpA, counselling has been associated with reduced postpartum flares and longer gestational age, despite similar antenatal disease activity, reinforcing its role in optimizing pregnancy timing, facilitating shared decision-making (SDM) and reducing preventable maternal and foetal risk in individuals with AIRDs.52
Multidisciplinary care models
Specialized multidisciplinary clinics integrating rheumatology and obstetric care consistently demonstrate improved pregnancy outcomes compared with fragmented models.8,43,44,53 A UK joint obstetric–rheumatology clinic reported 97% live births among 98 pregnancies in women with AIRDs, with 2% miscarriage, 1% stillbirth, a median gestational age of 38 weeks and a mean birth weight of 3,120 g, comparable to the general population, underscoring the impact of coordinated co-management.8 In the USA, a multidisciplinary clinic managing 84 high-risk AIRDs achieved 52% live births, with 25% PTB, reflecting the expected risk profile of the cohort, and required initiation or modification of pregnancy-compatible therapies in 52% of cases.54
Medication use based on evidence
Current reproductive health guidelines from the ACR, EULAR and BSR provide broadly aligned, evidence-based recommendations for medication use across reproductive stages in individuals with AIRDs (Table 3).5,6,28 The updated EULAR 2024 guidelines have adopted a more permissive, individualized approach to biologic use in pregnancy, reflecting accumulating safety data and emphasizing careful risk–benefit assessment to optimize maternal disease control, given the established association between uncontrolled inflammation and adverse maternal and foetal outcomes.5 Mechanistically, placental transfer of monoclonal immunglobulin-G (IgG)-based biologics via the neonatal fragment crystallizable (Fc) receptor begins after 20 weeks’ gestation and varies by molecular structure, being highest for monoclonal IgG1 antibodies, lower for Fc fusion proteins and negligible for Fc-free agents, forming the basis for trimester-specific treatment strategies.5 HCQ remains central to pregnancy management, particularly in SLE, with meta-analytic data demonstrating reduced disease activity and PTB without increased foetal risk.55–57 Similarly, registry and pharmacokinetic data support selective TNFi use, with certolizumab pegol showing minimal placental transfer and reassuring foetal safety.58,59
Unmet needs in reproductive rheumatology
Despite increasing recognition of reproductive health as a core component of care in individuals with AIRDs, substantial gaps persist across these diseases. Although major international societies have provided guidelines, their real-world implementation remains inconsistent, reflecting the voluntary nature of recommendations, predominantly low-certainty evidence and on-going structural and health-system-related barriers.7
A key limitation is the lack of standardized, lifecycle-oriented care pathways across reproductive stages (Figure 1). Fewer than 30% of centres report dedicated rheumatology–obstetric services, leading to wide variability in core practices such as contraception counselling for teratogenic therapies, postpartum flare risk assessment and longitudinal monitoring in nephritis. These inconsistencies are compounded by deficiencies in formal training, with surveys from India and the USA demonstrating low clinician confidence in counselling on fertility preservation and assisted reproductive technique (ART).7,54,56,60
Gender-specific and patient-level disparities further compound the issue. While male reproductive health in AIRDs is increasingly recognized, it remains underrepresented in current evidence. Emerging data suggest that paternal inflammatory arthritis itself may influence pregnancy outcomes, highlighting an under-recognized contributor to reproductive risk.61 Although guidelines address male reproductive risks, such as sperm banking prior to CYC exposure, there is still a lack of supporting evidence.5,6 Male subfertility related to disease and treatment, such as transient effects of NSAIDs, sulfasalazine-associated oligospermia and CYC-related gonadotoxicity, is underrecognized, and there are limited data on paternal exposure to newer targeted therapies.5,6 These factors highlight the need for structured counselling, fertility preservation techniques and individualized risk–benefit analysis.
Patient education is similarly inadequate, with approximately one-third of women reporting never receiving formal reproductive counselling, often relying on online misinformation.43
Finally, persistent evidence gaps constrain progress. Randomized controlled trials (RCTs) in pregnancy are lacking, long-term data on offspring of women with AIRDs remain limited, particularly for immune-mediated conditions such as congenital heart block (CHB) and neonatal lupus, and most data derive from high-income settings, limiting generalizability to low- and middle-income countries.1,3,17,18,23 Addressing these gaps will require coordinated structural solutions, including EMR-based prompts, integration of reproductive rheumatology into training curricula, disease-specific patient education resources and targeted research on male fertility and long-term offspring outcomes to advance equitable, evidence-based reproductive care in individuals with AIRDs.
Reproductive rheumatology continues to face critical evidence gaps across the reproductive life course in individuals with AIRDs. Priority areas include pregnancy-specific therapeutic safety, postpartum disease control, fertility and ARTs, male reproductive health and long-term offspring outcomes, particularly beyond the neonatal period.2 Conventional RCTs in pregnancy remain ethically and logistically constrained, resulting in reliance on observational and registry-based data, especially for rare or high-risk AIRDs such as ANCA-associated vasculitis and for newer biologic and targeted therapies with limited reproductive safety data.2,5
To address these challenges, innovative methodological approaches are required. Pragmatic registry-based studies, cluster-randomized designs and harmonized international datasets offer feasible alternatives to traditional trials, enabling comparative effectiveness and safety evaluations while minimizing ethical risk.3,5,11,12,42 The EULAR core pregnancy data set provides a framework for standardized data capture and pooled analyses across registries, facilitating robust evaluation of maternal, foetal and neonatal outcomes.11 Longitudinal cohort designs linking pregnancy registries with paediatric and rheumatology databases are essential to elucidate long-term neurodevelopmental, autoimmune and cardiometabolic outcomes following in utero exposure to immunomodulatory therapies.11,42
Role of registries
Existing registries
Pregnancy registries have become a central resource in reproductive rheumatology. National registers, such as the British Society for Rheumatology Biologics Register (BSRBR), now include pregnancy modules to track outcomes for women receiving specific therapies.62 Disease-specific registries, such as lupus pregnancy registries and antiphospholipid research cohorts, provide additional targeted insights.11 Many registries are increasingly incorporating structured data collection, with growing emphasis on long-term offspring follow-up to evaluate developmental outcomes.11
Value of registry-based real-world data
Pregnancy registries represent a cornerstone of real-world evidence (RWE) generation in AIRDs, enabling systematic evaluation of drug exposures and disease-related risks that cannot be ethically studied in RCTs.63 Large-scale European pregnancy registries, including RheKiss (German register for child wish and pregnancies in inflammatory rheumatic diseases) and the French “Grossesse et Rhumatismes Inflammatoires” (GR2) cohort, have become pivotal in advancing evidence-based reproductive rheumatology by providing robust longitudinal data on fertility, disease activity, medication safety and maternal–neonatal outcomes across major AIRDs.64–66 However, persistent ethical, regulatory and methodological challenges in pregnancy research necessitate innovative trial designs, adaptive methodologies and registry-based approaches to ensure high-quality evidence generation while safeguarding maternal and foetal safety.67 This is particularly relevant for early pregnancy exposures to teratogenic drugs such as methotrexate (MTX), underscoring the importance of effective contraception and preconception counselling.27,45,46,49 Observational database and pregnancy cohort studies suggest no consistent increase in congenital malformations with preconception or early methotrexate and TNFi exposure, providing reassurance.68,69 By pooling large longitudinal cohorts, registries also enable detection of rare outcomes, such as CHB in anti-Ro/La antibody-positive lupus and Sjögren’s disease pregnancies, with pooled estimates indicating a baseline risk of 3–5% and approximately 2% progression to complete heart block.27
Beyond individual drug safety signals, registries inform disease control and temporal trends in maternal and foetal outcomes. The aforementioned Italian registry reported maternal flares in 15.6% of pregnancies (highest in PsA) and documented an 84% live-birth rate, reflecting improved multidisciplinary care.12 Similarly, the recent Canadian data show a 24% increase in pregnancy rates among women with RA and PsA between 2011 and 2021.70
Registries also drive hypothesis generation and quality improvement. A study identified major gaps in contraception counselling among women receiving biologics, prompting EMR-based interventions that increased documentation from 11% to 54%.71 At a systems level, EULAR has enhanced registry interoperability through a standardized core pregnancy data set, harmonizing disease activity, medication exposure and APOs, and enabling rapid pooled analyses, including evaluation of Coronavirus disease 2019 (COVID-19) vaccine safety during pregnancy.11
Finally, pregnancy registries underpin post-authorization safety studies mandated by regulatory agencies such as the European Medicines Agency (EMA) and US Food and Drug Administration (FDA), facilitating quantification of rare outcomes, including neonatal lupus.3,11,64,66,72 Despite these advances, substantial gaps remain, particularly in underrepresented regions, rare or high-risk AIRDs, and newer biologic or targeted therapies with limited reproductive safety data.1,3,5,18,22,23,27,42,66 Continued expansion and global strengthening of RWE infrastructures remain essential to advancing equitable, evidence-based reproductive rheumatology care.
Collaborative and multidisciplinary approaches
Inter-specialty collaboration
Formal multidisciplinary management models have been shown to improve care delivery and outcomes for women with AIRDs.8,37,54 Shared-care protocols standardize foetal echocardiography for those with anti-Ro antibodies+, aPL monitoring for APS and postpartum flare prophylaxis for RA and SpA (40–50% risk), while also aiming to optimize long-term outcomes for children born to these patients.72–74 The ACR 2020 Reproductive Health Guidelines exemplify multidisciplinary consensus among rheumatologists, obstetricians and maternal–foetal medicine specialists.6
Patient partnership
International professional societies play an increasingly central role in advancing reproductive rheumatology through coordinated research, guideline development and patient engagement.5,6 In parallel, formal frameworks for patient partnership, including active patient involvement in research prioritization and study design, have strengthened the relevance, acceptability and translational impact of rheumatology research, reinforcing patient-centred care models at a global level.75,76
Patient partnership and SDM are integral to this framework and are explicitly endorsed by the ACR 2020 guidelines and the EULAR 2023 recommendations on patient research partners (PRPs).6,65,76 The EULAR PRP framework emphasizes systematic integration of patient perspectives into research, ensuring that outcomes meaningful to patients are considered alongside traditional clinical endpoints.65 Despite this endorsement, implementation remains variable. A 2021 global survey reported limited clinician familiarity with structured SDM models, frequent deferral of reproductive discussions to obstetric services and low confidence in contraception counselling, particularly for MTX-exposed and aPL-positive patients.57 Emerging evidence supports the effectiveness of SDM interventions, including digital decision aids and pregnancy planning tools, which facilitate individualized, evidence-based counselling aligned with patient priorities.46,77 Embedding structured SDM tools and expanding clinician training are therefore essential to translating global guidance and patient partnership into consistent, patient-centred reproductive care in individuals with AIRDs.
Future directions
Reproductive rheumatology is increasingly recognized as an emerging subspecialty, with anticipated development of dedicated training curricula and certification pathways within women’s health rheumatology. Integration of reproductive health into EMR systems offers a pragmatic opportunity to address current gaps, including automated prompts for contraceptive counselling in patients receiving teratogenic therapies and routine screening of pregnancy intention, which may improve persistently low observed documentation rates.48 Telemedicine platforms further expand access to preconception counselling and disease monitoring, particularly for patients in rural or low-resource settings, supporting continuity of care across reproductive stages.48,66,67
Technological advances are likely to enhance individualized risk stratification, including digital pregnancy-tracking tools integrated with rheumatology EMR and emerging biomarker strategies to predict complications such as PEC or CHB in high-risk pregnancies.2,66,67 Future research priorities extend beyond pregnancy outcomes to include long-term child development following in utero drug exposure, reproductive ageing and menopause-related disease trajectories in AIRDs, and paternal health outcomes, areas that remain insufficiently studied despite their clinical importance.19,20,57 From a health-policy perspective, preventive, multidisciplinary reproductive care is increasingly recognized as cost-effective, with reductions in APOs translating into substantial healthcare savings.1,8,10,22–24,43 The long-term vision is an integrated reproductive lifecycle model in which every reproductive-age individual with AIRDs receives anticipatory counselling at diagnosis and seamless multidisciplinary support from preconception through pregnancy, lactation and beyond.38
Conclusion
Reproductive rheumatology should be recognized as an integral component of routine care for individuals with AIRDs, rather than a discretionary subspecialty interest. Contemporary evidence indicates that APOs are driven predominantly by modifiable factors, including active disease, inappropriate medication exposure, delayed counselling and fragmented care, rather than by diagnosis of specific AIRD alone.1,5,6,8,23,25,31,39,42,44–46,50 With planned conception during disease quiescence, appropriate management of teratogenic therapies and multidisciplinary care, maternal and foetal outcomes can closely mirror those of the general population.5,6,8,24,25 Integrating structured reproductive counselling, guideline-aligned medication strategies and coordinated rheumatology–obstetric pathways into standard practice is therefore essential to translating improved survival in individuals with AIRDs into optimal reproductive health outcomes.











