
Virtual reality (VR) is an emergent technology with the potential for genuine impact as a novel, immersive digital therapeutic in healthcare. Within rheumatological conditions, pervasive symptoms including chronic pain and kinesiophobia (fear of movement) are difficult to manage using conventional non-pharmacological methods, highlighting the need for innovative, home-based approaches. This article summarizes the current research evaluating therapeutic VR in rheumatology, including developments related to chronic low back pain (cLBP), chronic neck pain (cNP), complex regional pain syndrome (CRPS), fibromyalgia syndrome (FMS) and other rheumatological diseases such as rheumatoid arthritis (RA).
Virtual reality in healthcare
VR is a novel technology that uses a head-mounted display (HMD) to provide full audiovisual immersion by encapsulating users within an interactive, 360 degree virtual environment. Modern VR systems are technically sophisticated and include a range of cameras and sensors to track the user’s physical surroundings, movements and even physiological responses. Interaction with elements of the virtual environment is enabled through tracked handheld controllers or, increasingly, direct hand tracking. In recent years, lower-cost consumer-available systems have made VR an accessible and scalable home-based option with the potential to address pressing healthcare needs.
Therapeutic VR is supported by established evidence across a diverse range of physical and mental health conditions.1,2 For example, in acute pain management, immersive VR activities significantly reduce pain perception by redirecting attention and promoting relaxation.3,4 Beyond this, VR’s capacity to influence sensory and cognitive experiences through attentional modulation, embodiment (the sensation of owning a virtual body), graded movement and mind–body approaches positions it as a novel multi-modal tool for managing complex health conditions.
Beyond its mechanistic value, VR’s scalability and adaptability make it particularly suitable as a home-based, person-centred therapeutic option to complement traditional management.5,6 In rheumatology, where many conditions are multifaceted and chronic, VR has the potential to enhance self-management and improve outcomes.
Complementing non-pharmacological approaches in rheumatology
Rheumatological conditions such as inflammatory arthritis and FMS are characterized by chronic pain, functional impairment and psychophysical challenges such as kinesiophobia. Despite advancements in pharmacological therapies, many patients still experience suboptimal symptom relief with lasting impacts on their quality of life.
Non-pharmacological interventions play an essential role in the management of rheumatological conditions, particularly in addressing chronic pain and promoting physical function. Approaches such as physiotherapy and psychological therapy (such as cognitive-behavioural therapy) are evidence-based and widely used.7,8 However, adherence and accessibility remain significant barriers, particularly within a resource-constrained healthcare system such as the National Health Service (NHS). The need for cost-effective and accessible solutions that can overcome these challenges is evident, driving interest in emerging modalities such as therapeutic VR.
Purpose of this review
Therapeutic VR is a rapidly evolving field, offering promising applications across healthcare. Within the context of rheumatology, research remains in its early stages. This structured narrative review aims to describe and summarize the current evidence on therapeutic VR in rheumatology, discuss opportunities in the field and identify gaps to guide future research. By exploring the potential of VR across the spectrum of rheumatological diseases, this article highlights its emerging role in advancing patient-centred care.
Methodology
This narrative review was conducted following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines.9 A protocol was not registered for this study.
Search strategy
For our narrative review, a systematic search was conducted using MEDLINE (OVID) and Embase (OVID) databases, covering publications from 1 January 2000 to 12 January 2025. This date range was chosen to capture studies using modern VR hardware over a 25-year period. The search combined Medical Subject Headings (MeSH) terms and free-text keywords related to rheumatological diseases, VR technologies and primary research study designs. Boolean operators were used to link these terms and identify primary research studies on VR applications in rheumatological diseases (Supplementary Table S1).
Study eligibility
Primary research studies involving human participants and focusing on VR-based therapies for rheumatological diseases were included. Studies using VR for non-therapeutic purposes (such as education) without a reference to improving patient outcomes were excluded. Studies using non-immersive forms of VR without the use of a HMD were also excluded. To maintain a focus on rheumatology-specific applications, we excluded studies involving postsurgical or orthopaedic populations (e.g. fracture cases) and those with general ‘chronic pain’ cohorts that lacked reference to specific rheumatological conditions. Manuscripts reporting incomplete data, conference papers and letters to the editor were excluded. Only English-language publications were included to maintain interpretative consistency.
Study screening and data extraction
Titles and abstracts identified through the literature search were uploaded to Rayyan, an online tool for systematic review screening, where deduplication and abstract screening were conducted by Jordan Tsigarides (JT).10 Screened citations were exported to EndNote 20 (Clarivate, Philadelphia, PA, USA) for full-text review. Full-text screening was completed by JT, and reference lists of eligible studies were manually checked for additional relevant studies. Independent review by Nicholas Fuggle (NF), Benjamin Kannuralil Sabu (BS) and Samuel Hughes (SH) confirmed that selected studies met the eligibility criteria. Disagreements or uncertainties regarding study eligibility were resolved through discussion to reach consensus. Although inter-rater agreement statistics were not calculated, this collaborative process helped ensure consistency and rigour. Data extraction by JT captured information such as lead author, year of publication, journal, study title, cohort(s) studied, outcome measures, VR technologies used and key results. Data were extracted into a structured Microsoft Excel spreadsheet (Microsoft, Redmond, WA, USA).
Data synthesis
A structured narrative synthesis was conducted in line with the Economic and Social Research Council’s ‘Guidance on the Conduct of Narrative Synthesis in Systematic Reviews’.11 This synthesis examined therapeutic VR applications in rheumatological diseases, focusing on intervention types, study populations and clinical outcomes, including patient-reported measures such as pain and quality of life.
While this study followed PRISMA guidelines, formal quality appraisal using tools such as GRADE was not undertaken. This decision was made due to the considerable heterogeneity in study designs, interventions, outcomes and the narrative nature of the synthesis. Instead, relevant study characteristics including design, sample size, VR modality, comparators, session frequency and outcome measures are reported consistently to allow readers to interpret findings in context. The synthesis aimed to provide an overview of therapeutic VR’s potential in rheumatology, highlighting both established evidence and areas for further investigation.
Results
Overall study characteristics
This study included 56 studies investigating VR interventions across a range of rheumatological conditions (see Figure 1). Most studies investigated cLBP and cNP, with smaller numbers investigating CRPS, FMS and others including RA and osteoarthritis (OA). The earliest study was published in 2010, with the majority (78%) published between 2020 and 2025. Study designs varied widely, with randomized controlled trials (RCTs) being the most common. Other methodologies included pilot studies, crossover designs, cross-sectional studies, mixed-methods and qualitative research. VR approaches varied by condition and included embodiment, graded exposure, exergames, guided meditation, attentional modulation, sensorimotor training and multimodal interventions (see Table 1).
Figure 1: PRISMA 2020 flow diagram
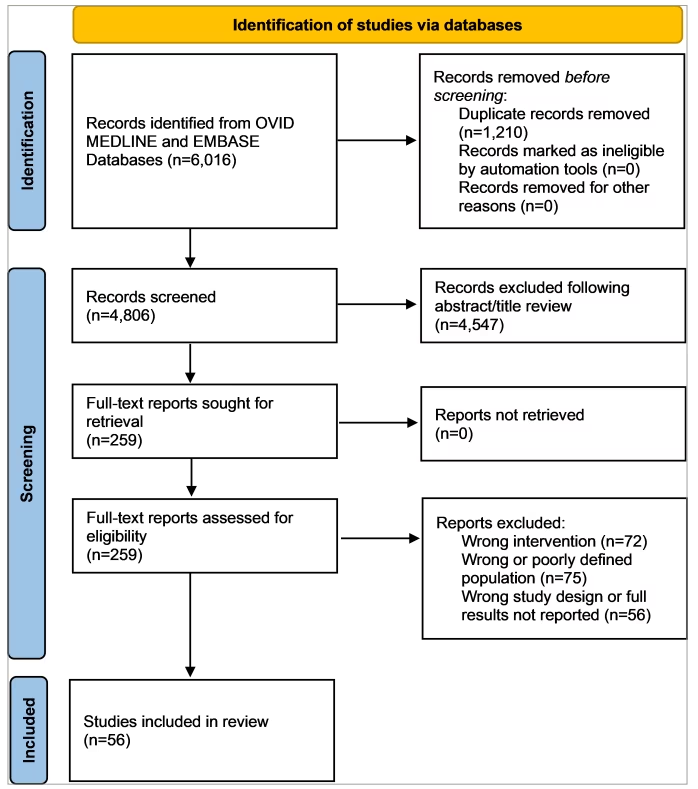
Table 1: Summary of included studies by condition: Study design, sample size and virtual reality approaches
| Cohort | Number of studies | Design(s) | Median sample size (IQR, range) | VR approach(es) |
| cLBP | 21 | RCT, cohort, qualitative and single-case experimental | 52.0 (138.0, 10–1,093) | Multimodal, embodiment, graded exposure, exergames, CBT, movement therapy and pain neuroscience |
| cNP | 13 | RCT, cohort, cross-sectional and within-subjects experimental | 41.0 (31.0, 19–75) | Kinematic training and measurement, visual feedback and sensorimotor training |
| CRPS | 6 | Pilot, RCT and crossover | 14.5 (13.5, 8–39) | Embodiment, guided visualization, mirror therapy and biofeedback |
| Multiple | 6 | Pilot, randomized-crossover, RCT, mixed-methods, and non-randomized interventional | 27.0 (30.8,12–97) | Multimodal, attentional modulation, motor imagery, embodiment, relaxation, guided meditation and biofeedback |
| FMS | 4 | RCT, randomized crossover and feasibility | 35.0 (31.8, 16–89) | Attentional modulation, balance and mobility training, guided movements and embodiment |
| Shoulder pain | 2 | RCT | 42.0 (6.0, 36–48) | Gamified range of motion and strength training, and virtual functional tasks |
| RA | 1 | Pilot | 13.0 | Guided meditation |
| OA | 1 | Feasibility | 19.0 | Guided meditation |
| CTS | 1 | Feasibility | 10.0 | Sensorimotor training |
| Chronic leg pain post-SCS | 1 | Non-randomized interventional | 15.0 | Visual feedback training |
CBT = cognitive behavioural therapy; cLBP = chronic low back pain; cNP = chronic neck pain; CRPS = complex regional pain syndrome; CTS = carpal tunnel syndrome; FMS = fibromyalgia syndrome; IQR = interquartile range; OA = osteoarthritis; RA = rheumatoid arthritis; RCT = randomized controlled trial; SCS = spinal cord stimulator; VR = virtual reality.
Chronic low back pain
Overview
cLBP is a common condition characterized by persistent pain affecting the lower back lasting over 3 months. It often leads to functional disability, kinesiophobia and mood disturbances. Underlying mechanisms may include central sensitization and altered movement patterns. There has been increasing interest in the use of VR to support the physical and cognitive aspects of symptom management.
Study populations and study designs
A total of 21 studies (2017–2024) investigated the effects of various VR interventions on individuals with cLBP.12–32 Two studies also included individuals with neck pain.24,28 A variety of study designs were used, including RCTs, cohort studies, qualitative studies and single-case experimental designs.12–32 Sample sizes varied widely (ranging from 10 to 1093), with a median sample size of 52. Four studies reported longitudinal follow-up data related to other studies included in this article.15,16,26,27
Types of VR interventions
A range of different VR interventions was used to target one or more elements associated with chronic pain (e.g. pain intensity, pain interference, kinesiophobia, disability, quality of life and physical function). Several studies used multi-modal, skills-based programmes incorporating pain education, relaxation, mindfulness and CBT techniques.15–18,23,25–27,29 These typically involved daily sessions over several weeks and aimed to build coping and self-management strategies. One programme used a similar approach but prioritized embodiment within a broader therapeutic framework.14
In contrast, one study used a distinct category of intervention the authors called VR neuroscience-based therapy (VRNT), which specifically integrated pain neuroscience education with neurocognitive and CBT-based activities within immersive environments.22 Other studies focused more explicitly on embodiment-based interventions, such as body ownership illusions.20,21,28 Additional interventions targeted physical activity or VR exergaming, which combines physical exercise with engaging game-like elements in VR.13,19,30–32
Comparators
Most studies used active or passive control conditions. Waitlist control groups were used in some studies to explore the effects of VR beyond spontaneous improvements.18,22 Sham VR interventions were adopted in others, including delivery of the same VR setup without therapeutic content or exposure to 2D videos and neutral VR environments.14–17,21,25–28 These sham interventions aimed to isolate the specific therapeutic components of VR such as embodiment, interactivity or immersion by controlling for non-specific effects including VR system novelty, visual stimulation or participant expectation. Some studies also compared VR to standard care, such as conventional physiotherapy, medication or CBT.14,18,21,29,30
Key findings
Overall, the findings of the reviewed studies suggest that, depending on the type of VR intervention used, these therapies may be effective in reducing pain intensity, fear of movement and disability while improving quality of life, physical function, body image and self-efficacy in people with cLBP.
Notably, several studies included large sample sizes, home-based delivery and/or longitudinal follow-up. In a double-blind RCT (initial study n=179), an 8-week, skills-based, multimodal VR programme delivered in a home setting led to improvements in function, with durable reductions in pain intensity and interference lasting up to 24 months.15–17,27 A separate larger RCT (initial study n=1093) reported sustained reductions in pain intensity and interference at 12 months with a skills-based VR intervention, and a UK-based RCT using a multi-modal embodied VR intervention (n=42) demonstrated improvements in disability and pain interference at 5-month follow-up.14,25,26 These findings reinforce the feasibility and long-term benefits of VR in cLBP.
Similarly, a behavioural skills-based programme with shorter follow-up duration demonstrated improvements in pain and function, with virtual CBT demonstrating improvements in depression and anxiety symptoms.18,24
VRNT improved pain intensity and quality of life, with neuroimaging-based outcomes suggesting positive alterations in central networks linked to chronic pain.22 VR has also been shown to be a feasible and safe approach for exercise-based therapies.28 Improvements in pain, kinesiophobia and physical function (measured through improved trunk velocity during bending) were also demonstrated through VR game-based exposure therapy and exergaming interventions.13,30,32 VR training also improved postural sway, balance and functional performance in older women with cLBP.31
Embodiment interventions led to improvements in body image and self-efficacy, including reduced pain following superhero embodiment and single-session body image re-training.12,21 Graded VR exposure programmes were both feasible and effective in increasing activity levels and reducing kinesiophobia.19,20 High feasibility and participant satisfaction were reported in a study integrating VR-based pain neuroscience education with physiotherapy.29
Conclusion
VR has the potential to deliver a diverse range of interventions in one virtual space that show promise in managing cLBP. Studies completed to date highlight the potential of different VR interventions to reduce pain, improve physical function, decrease kinesiophobia and enhance body image. Longitudinal findings from recent home-based studies support the potential for durable benefits. Future research should explore the optimal integration of biopsychosocial pain management programmes with VR and should focus on evaluating long-term impacts across real-world settings.5
Chronic neck pain
Overview
cNP is a common musculoskeletal condition characterized by persistent pain affecting the neck lasting over 3 months. It presents with reduced cervical range of movement (CROM), movement-related pain and postural alteration. Central sensitization and fear-avoidance behaviours may also contribute to the condition. VR has been explored for both movement assessment and therapeutic rehabilitation in people with cNP.
Study populations and study designs
A total of 13 studies (2010–2023) examined the impact of VR interventions on cNP.24,28,33–43 Two studies also included individuals with cLBP.24,28 Study designs used include RCT, cohort studies, cross-sectional and within-subjects experimental.24,28,33–43 Sample sizes varied (19–75 participants), with a median sample size of 41.
Types of VR interventions
Interventions ranged from targeting motor control and proprioceptive feedback to interactive games aimed at improving cervical kinematics. Two studies used VR to immerse and distract participants while they completed traditional cervical movement exercises.41,43 One of these studies used a gamified approach using tracking of head and neck movement through the HMD.43 One study used VR to determine whether altering visual-proprioceptive feedback associated with cervical movements influenced the range of motion that participants could tolerate before the onset of pain.35 Four studies assessed the accuracy of VR in assessing cNP disability through measurement of CROM.36,38,40,42
Comparators
For studies evaluating the utility of VR to measure CROM, VR-based systems were benchmarked against either conventional goniometry or gold-standard marker-based motion capture, with the goal of identifying if VR could act as an objective tool.38,40,42 Rehabilitation studies that used VR to improve CROM used supervised conventional exercise therapy comparators such as in-person physiotherapy to assess feasibility of remote VR therapy.37,39,43 One study that aimed to assess the role of fear-avoidance in CROM simply compared altered visual cues using VR with no visual feedback manipulation.35
Key findings
Overall, the findings of the reviewed studies suggest that VR may be effective in reducing pain intensity, disability and kinesiophobia, while improving CROM, proprioceptive function and psychological wellbeing in people with cNP.
An RCT (n=41) found that integrating VR into motor control exercise significantly improved pressure pain thresholds at C1/C2 and C5/C6, reduced kinesiophobia and increased exercise compliance compared to conventional motor control exercise alone.33,34 A further RCT (n=44) reported that immersive VR exercise led to greater reductions in kinesiophobia than conventional physiotherapy, with effects maintained at 3-month follow-up.43 Additionally, a pilot RCT (n=32) comparing cervical kinematic training with and without immersive VR found that both groups improved in disability, CROM and movement velocity, with the VR group reporting greater satisfaction and global perceived benefit.41
A further pilot RCT (n=51) compared neck-specific VR sensorimotor training to general sensorimotor training and standard rehabilitation. The VR group demonstrated greater improvements in CROM, headache severity and self-reported disability compared with standard rehabilitation and also improvements in cervical extension compared to general sensorimotor training, exceeding minimal clinically important differences for several outcomes.40
VR was also used to manipulate visual feedback and modulate pain-free range of motion. One study showed that understating head rotation in the VR display by 20% enabled participants to rotate their heads 6% further before pain onset.35 Similarly, another study found that altered visual feedback led to increased CROM and reduced kinesiophobia, especially when the rotation was visually understated.37 In contrast, a different study found no significant effects when stratifying participants by pain duration (n=71), although a more recent study using refined methods and more rigorous exclusion criteria (n=75) demonstrated increased pain-free CROM with understated visual feedback in those with higher fear-avoidance beliefs.38,39
Psychological and functional outcomes were also addressed using a remote approach with home-based cognitive behavioural therapy delivered through VR. A 14-week programme (Harvard MedTech Vx Pain Relief Program (Vx therapy), n=63) resulted in significant improvements across Patient-Reported Outcomes Measurement Information System (PROMIS) domains for pain intensity, interference, behaviour, anxiety and depression.24 In another retrospective analysis (n=82), delivery of exercise therapy in the ‘metaverse’ led to a significant 23.2% reduction in Neck Disability Index scores, with no adverse effects reported.28
Lastly, several studies established the validity of VR for movement assessment. VR-derived CROM measures correlated well with conventional goniometry and marker-based motion capture, supporting its potential utility as a clinical tool for neck function assessment.36,42
Conclusion
VR interventions show promise in the management of cNP by improving pain, motor control and CROM. Studies suggest that immersive environments and manipulation of visual-proprioceptive feedback can enhance rehabilitation outcomes. Despite positive findings, limitations such as small sample sizes and technological variability highlight the need for larger, standardized trials to fully establish VR’s role in the rehabilitation of cNP.
Complex regional pain syndrome
Overview
CRPS is a chronic pain condition involving severe, disproportionate pain following an inciting event such as trauma or surgery. Although mechanisms remain unclear, central and peripheral nervous system dysregulation, inflammatory responses and altered body perception are thought to contribute. Symptoms include motor, sensory and autonomic changes such as oedema and temperature dysregulation. VR has been explored to modulate body schema, reduce pain and improve motor function in CRPS.
Study populations and study designs
Six studies (2014–2021) investigated the use of VR in CRPS, primarily type I.44–49 Study designs included randomized controlled and uncontrolled pilot studies, cross-sectional and crossover.44–49 Participants were mainly recruited from outpatient rehabilitation services and pain management centres. Sample sizes were small across studies (range 8–39, median 14.5). A total of 68 participants with CRPS (age 42.9 ± 3.9 years; male:female 39:29) across these studies undertook a VR intervention.
Types of VR interventions
Most studies used embodiment in VR to manipulate body representation and perception in patients with CRPS.45–49 These interventions attempt to improve pain perception and reduce body perception disturbance using various mechanisms:
-
The Mirror Visual Feedback intervention aims to correct disrupted body schemas and reduce pain through VR adaptations of traditional mirror therapy.49
-
The Body Swapping Illusion intervention induces a sense of ownership over a virtual body, usually involving mental rehearsal, where participants mentally synchronize their movements with those of a virtual body.45,46
-
Visual body manipulation interventions include altering the visual characteristics of a virtual representation of the affected limb. This includes cardiovisual stimulation where participants view the affected limb flashing in synchrony with their heartbeat, or various alterations in transparency and size of the virtual limb.47,48
One study took a different approach and used VR as an interactive functional intervention, incorporating simulated activities of daily living that required participants to visualize and manipulate virtual objects through grasping, sorting, assembling and following movement patterns.44
VR session lengths ranged from 10 to 60 minutes. Most studies tested feasibility or immediate effects with single sessions, while others used multiple sessions over several weeks.44–49
Comparators
Most studies employed either within-subject or parallel group designs to compare intervention and control conditions.45–48 Control conditions often included similar VR setups lacking key intervention elements. For example, asynchronous feedback instead of synchronized heartbeat-enhanced VR, or watching movement without any mental rehearsal.45–47 Two pilot studies lacked explicit control conditions and instead explored feasibility and subjective outcomes.44,49
Key findings
VR interventions for CRPS showed mixed results. Four studies reported reductions in pain intensity following VR interventions, with some patients experiencing a significant decrease after a single session.45–48 One study demonstrated a potential influence of synchronizing visual elements of the affected limb with the heartbeat, with significant improvements in pain compared with an asynchronous condition which also improved function and modulated heartrate variability.47 In contrast, two studies showed no significant change in pain scores.44,49
Improvements in body perception disturbance were observed across the two studies using body swapping VR interventions, suggesting VR may help to normalize disrupted body schema.45,46 One study found that increasing transparency of a virtual representation of the affected limb significantly reduced pain in CRPS, but not in those with peripheral nerve injury, whilst increasing limb size in CRPS increased pain ratings.48 This perhaps highlights the importance of tailoring visual feedback to the patient group.
VR interventions were generally well tolerated, with minimal adverse effects reported in one feasibility study.49
Conclusion
VR interventions show promise as a non-invasive approach to manage the complex symptoms of CRPS and target underlying body perception disturbances. However, small sample sizes, outcome variability and study heterogeneity limit current evidence. Further research is needed to establish VR’s potential as a flexible, engaging and customizable treatment option for CRPS.
Fibromyalgia syndrome
Overview
FMS is a chronic pain condition affecting between 4 and 6% of the adult population and is characterized by chronic widespread pain, excessive fatigue, unrefreshing sleep and other associated somatic symptoms. Central and peripheral sensitization are key mechanisms. VR has been studied to support movement, alter attentional resource allocation and promote mindfulness in people with FMS.
Study populations and study designs
Four studies (2022–2025) investigated outcomes related to various VR interventions in FMS.50–53 Heterogeneity in study design was present across the studies, with designs including feasibility, randomized-crossover and RCTs. Sample size varied between studies, with a median sample size of 35.0 (range 16–89).
Types of VR interventions
VR was used for different purposes across the four studies. Two studies used interactive VR activities to promote attentional modulation one used VR for balance and mobility training and one used VR to support guided movements delivered by a mirror-like avatar in combination with a neuromodulation EXOPULSE Mollii suit (Exoneural Network AB, Danderyd, Sweden).50–53
Comparators
Comparators were used in most studies (n=3) to measure the effects of VR compared with control conditions.50,52,53 One study compared a cold-pressor task alone (control) with the same task combined with VR in a cross-over design to evaluate the impact of VR on pain outcomes, including pain thresholds and tolerances.50 Another study compared the effects of an 8-week aerobic and Pilates exercise regime alone (control) with the same regime that included additional use of VR, investigating outcomes related to pain, movement and quality of life.52 A further four-arm study evaluated psychophysiological outcomes by comparing the use of the EXOPULSE neuromodulation suit alone, the suit combined with VR and an exercise regime alone, against a control group using an inactive EXOPULSE suit.53
In contrast, one uncontrolled feasibility study took a different approach and compared different VR systems, activities and virtual environments to evaluate differences in acceptability (including adverse effects) and impact on clinical outcomes across intervention characteristics.51
Key findings
Overall, the review findings highlight early but growing evidence supporting the use of therapeutic VR in FMS. The reviewed studies demonstrate the feasibility of VR and its potential to improve both pain and psychological outcomes.
Interactive attention-based VR demonstrated strong acceptability and low adverse effects in FMS across a range of consumer VR systems (Samsung Gear VR, Oculus Go, Quest and Rift), four VR activities and two virtual environments (cold and warm).51 Participants with FMS reported overwhelmingly positive perceptions of VR, particularly regarding openness to future use in their pain management, alongside improvements in both pain intensity and mood post-VR. However, variability in acceptability and clinical outcomes was noted across different VR systems and environments, highlighting the need to tailor VR interventions to the unique needs of FMS populations.
During a cold-pressor task, an interactive VR application delivered using the Oculus Rift S (Oculus VR, Meta Platforms Inc., Menlo Park, CA, USA) significantly increased cold pain threshold and pain tolerance compared to control.50 VR did not influence pain catastrophizing, and only reduced pain intensity for healthy participants. These findings suggest a possible role for interactive VR attentional modulation in altering pain thresholds and tolerances in FMS, though they contrast with other studies regarding VR’s impact on pain intensity.
The use of VR integrated with aerobic and pilates exercises over an 8-week period significantly reduced pain intensity, decreased kinesiophobia, improved fatigue and the mental component of quality of life compared to exercise alone.52 These findings highlight the potential of VR as an adjunctive tool in physical rehabilitation for FMS with enhanced benefits over traditional exercise programmes – the current gold-standard non-pharmacological treatment for FMS.
VR combined with the EXOPULSE neuromodulation suit demonstrated a greater reduction in pain intensity compared with the use of the suit or exercise alone.53 These results suggest a potential synergistic effect of combining neuromodulation and VR, although findings require replication in larger adequately powered studies.
Conclusion
Therapeutic VR shows promise in supporting the management of FMS, with evidence supporting feasibility and improvements in pain and psychological outcomes. However, the limited evidence base, small sample sizes and variability in interventions highlight the need for larger, long-term studies and real-world evaluations to truly understand VR’s role in FMS.
Other rheumatological diseases
Overview
This section will explore the literature surrounding the use of VR in RA, OA, carpal tunnel syndrome (CTS), shoulder pain (due to impingement or capsulitis), chronic leg pain following spinal cord stimulator (SCS) insertion and rheumatic disorder-specific chronic pain. These diseases involve persistent pain, joint dysfunction and psychosocial distress. VR has been used to support a range of approaches in these diverse rheumatological contexts.
Study populations and study designs
A total of 12 studies (2016–2025) investigated VR interventions across the conditions reviewed.54–65 These were early stage, pilot or feasibility studies with designs including single-arm, cross-sectional, randomized within-subject crossover, within-subject pretest–posttest and RCTs.54–65 Sample sizes varied but were small, with the largest study investigating rheumatology disorder-specific chronic pain (n=97) and the smallest investigating CTS (n=10).55,60 The majority of studies were for those with a mean age of about 50 years, with some including broad age ranges (18–75) and others focussing on older adults aged nearer to 70 years.54–59,61,62,64,65
Types of VR interventions
VR interventions included interactive VR exercise programmes including a climbing activity for frozen shoulder, immersive swimming and owl flying for shoulder impingement, guided meditations including nature-based environments for RA and OA, VR combined with sensorimotor activation (via vibrotactile cues) for CTS and VR visual body feedback for SCS-induced paraesthesia.56,57,60,61,64,65
The interventions for rheumatic disorder-specific–chronic pain studies included immersive-seated VR games for older adults (ranging from virtual travel to interactive music games), relaxation and meditation skills-based content, attention-based activities, immersive nature-based environments, virtual embodiment with grasping activities whilst measuring shoulder movement and meditation with respiratory feedback.54,55,58,59,62,63
The duration of VR ranged from 20 sessions over 4 weeks, with each session lasting 30 minutes to a single session lasting only 5 or 10 minutes.56,59,65
Comparators
Seven studies did not include comparators or control groups.54,57,59,60,62,63,65 In rheumatic disorder-specific–chronic pain studies, the comparators were an audio-only intervention (which included meditative narration) and non-immersive 2D video or audio-guided mental imagery.55,58 In the frozen shoulder study, the control group received electrotherapy and conventional shoulder exercises, and in the shoulder impingement study, the control group also received shoulder exercises and a home exercise programme.56,61 In the study of chronic leg pain following SCS, the VR congruent with SCS intervention was compared to incongruent SCS-VR and VR alone.64
Key findings
In the frozen shoulder study, VR appeared to produce a greater reduction in pain VAS compared to the electrotherapy and conventional exercise group, and the VR group showed greater improvements in shoulder ROM and pain scores compared to the controls in the study of shoulder impingement.56,61 While these randomized studies are promising, both studies were small and exploratory in nature.
The VR intervention in RA led to reduction in fatigue, depression and anxiety and also increased mood and physical function with high acceptability.57 Similarly, a small pilot study in CTS showed high usability of VR but with only moderate ratings for improvement in hand function and ease of use.60 In OA, one feasibility study reported a reduction in knee and overall pain following a VR meditation intervention.65
In the small study of chronic leg pain post-SCS, the congruent SCS-VR was associated with 1.8 times greater analgesic effect on average than the incongruent SCS-VR (and greater than the VR alone without feedback).64
In the studies of rheumatic disorder-specific–chronic pain, a 21-day course of VR meditation led to a greater reduction in pain intensity than an audio-only intervention, and reductions in pain intensity were observed after a single, 5-minute session.55 Pain reduction was also observed pre- to post-test for a virtual embodiment intervention.63 Nature-based VR interventions increased both pain detection threshold and pain tolerance thresholds more than non-immersive interventions, and nature-based visuals were associated with reductions in pain VAS when combined with either respiratory biofeedback or guided meditation, though the reduction in anxiety was greater with guided meditation than biofeedback.58,62 In older adults, 12 sessions including the use of various seated VR games over 6 weeks were associated with a decrease in pain (pre- to post-test).54
Conclusion
The current literature, though limited by sample sizes and lack of control groups (which are inherent to feasibility or pilot studies), do indicate potential efficacy with the use of VR in the management of RA, OA, CTS, shoulder pain (due to impingement or capsulitis) and chronic leg pain following SCS and rheumatic disorder-specific–chronic pain. These promising early findings warrant further investigation in larger, controlled studies.
Challenges, recommendations and future directions
This study highlights a rapidly growing body of literature investigating VR interventions across a broad spectrum of rheumatological conditions. While the approach is promising, several important limitations and challenges remain. Most studies to date are early phase conducted in small, non-diverse samples with limited follow-up durations. The heterogeneity of VR hardware, software platforms, intervention content, outcome measures and comparator groups further complicates synthesis and reduces the generalizability of findings.
Many interventions were delivered in controlled, lab-based or clinical settings, limiting understanding of their real-world utility, particularly as VR therapeutics are expected to support the shift from secondary care to community and home-based interventional delivery. Few studies evaluated cost-effectiveness, implementation challenges or barriers to home use, and key considerations in the broader move towards digital therapeutics and remote healthcare models. In addition, issues of digital equity and accessibility are underexplored. Older adults, individuals with limited digital literacy and socioeconomically disadvantaged populations may face unique barriers to engaging with VR-based therapies. Ensuring that interventions are co-developed alongside individuals with lived experience and inclusive by design is essential to avoid exacerbating health inequalities as digital therapeutics become more widely adopted. Furthermore, mechanisms underpinning VR’s therapeutic effects remain underexplored and require formal investigation using mixed-methods, biomarkers and neuroimaging.
Despite these challenges, several studies demonstrated high feasibility, acceptability and meaningful clinical improvements. Notably, recent large-scale RCTs using home-based, multimodal VR programmes in cLBP have shown sustained improvements in pain and function for up to 24 months. These findings support the real-world scalability of VR and its potential role in long-term symptom management.
To progress the field, future research should prioritize adequately powered, multicentre RCTs using condition-specific and standardized outcome measures. The development of core outcome sets for VR interventions in musculoskeletal and rheumatological conditions would enhance consistency and rigour across studies. Equally important is the inclusion of formal economic evaluations in larger trials to aid understanding of the real-world value of VR for routine clinical care and commissioning. Pragmatic trials are also needed to assess the effectiveness of VR in hybrid and home-based delivery models, reflecting how these technologies are likely to be used in practice. Studies should also explore factors that influence engagement, such as digital literacy, pain phenotype and patient preferences.
As VR technologies continue to evolve, the integration of artificial intelligence (AI), wearable biosensors and more sophisticated sensorimotor feedback provides new opportunities for developing responsive, closed-loop systems that adapt content in real time. Such innovations could enable truly personalized digital therapeutics delivered at scale in the community.
Therapeutic VR holds substantial potential to complement and enhance biopsychosocial models of care in rheumatology. With continued innovation, rigorous validation and user-centred design, VR may shift from an experimental adjunct to an integral component of long-term, person-centred care.
Conclusion
Therapeutic VR is an emerging and adaptable tool with promising applications across a range of rheumatological diseases. Early evidence highlights its feasibility, safety and potential to improve pain, physical function and psychological wellbeing. While the current evidence base remains limited by small sample sizes and heterogeneity, more robust studies such as those conducted in cLBP demonstrate encouraging long-term outcomes. As VR technologies continue to evolve, their integration into routine care may offer accessible, scalable and patient-centred solutions to complement existing non-pharmacological strategies in rheumatology.











