
Digital health encompasses technologies such as mobile apps, telemedicine, wearables, software and artificial intelligence (AI) that enhance remote, efficient healthcare delivery.1,2 In rheumatic and musculoskeletal diseases (RMDs), these tools address the need for continuous monitoring, early intervention and patient engagement.3,4 The coronavirus disease 2019 (COVID-19) pandemic dramatically accelerated their adoption and acceptance across care settings.5,6
The second most important development was the launch of various large language models (LLMs) that have highlighted the potential power of AI-based systems and started the worldwide race for the development of AI-based solutions. AI is already a part of our lives, and it is going to be indispensable in the near future.7
This review article explores how digital tools have impacted the world of rheumatology. The scope of the study is to provide a contemporary snapshot of available technologies to the rheumatologist. The first part deals with digital tools most of us have already heard of. However, the second part covers more operational software and solutions that are much more pragmatic and financially viable and are being used by institutions around the world to optimize patient care, including reducing patient wait times, optimizing laboratory utilization and showing tangible benefits. The conceptual framework illustrating how digital health tools intersect across the journey of patients with RMD from symptom onset to long-term management is depicted in Figure 1.
Figure 1: Framework: digital health tools across the journey of patients with rheumatic and musculoskeletal diseases
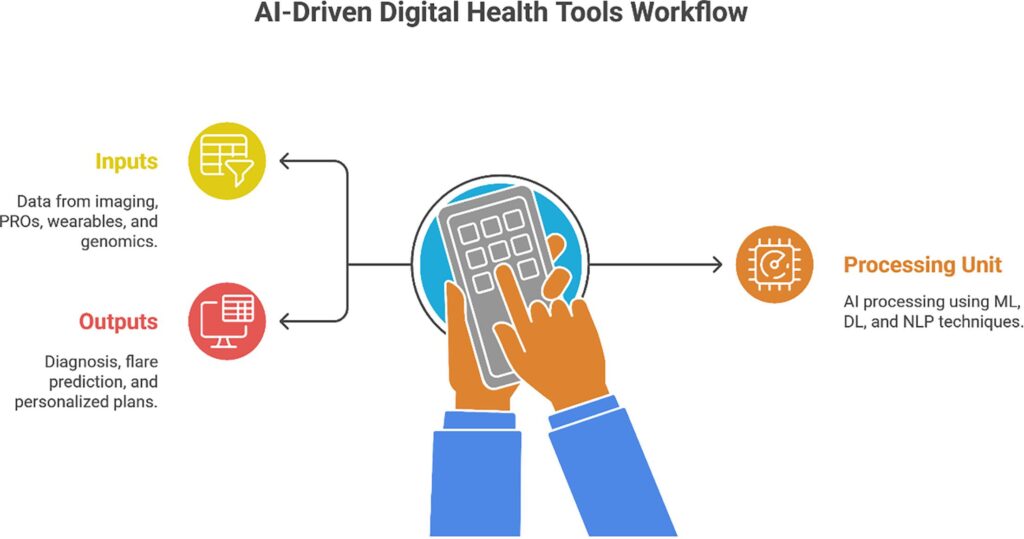
Figure 1 was created using Napkin AI (Napkin AI Inc., San Francisco, CA, USA) and Microsoft PowerPoint (Microsoft Corporation, Redmond, WA, USA). AI assistance was used solely for figure layout and visual presentation; all scientific content was conceptualized and verified by the authors.
AI = artificial intelligence; DL = deep learning; ML = machine learning; NLP = natural language processing; PROs = patient-reported outcomes.
Search strategy
We searched the literature on digital tools in medicine and their applicability to rheumatology, particularly in Scopus, MEDLINE (via PubMed) and Web of Science. We have manually screened and chosen articles that we found relevant, as per standard recommendations for writing biomedical narrative reviews.8
We have divided the article into two major sections: the first dealing with patient-facing and clinical applications and the second dealing with operational and management solutions based on AI. Discussion on the underlying AI algorithms is beyond the scope of this article. However, most of the work done to date remains based on LLMs.
Patient-facing and clinical support tools
The first part of the article examines 13 categories of patient-facing and clinical digital tools, including telemedicine, remote monitoring, diagnostic solutions such as clinical decision support systems (CDSS) and imaging-based diagnostics, as well as applications in drug development and precision medicine.2,9 An overview of these digital health tool categories, representative examples and their primary clinical applications in RMDs is provided in Table 1. To summarize the available evidence from systematic reviews and clinical trials across these domains, a consolidated overview is presented in Table 2.1,3,5,10–14 While Tables 1 and 2 summarize tool categories and clinical evidence respectively, Figures 1 and 2 provide a conceptual and outcome-oriented synthesis that integrates these findings across the patient care continuum.
Table 1: Overview of digital health tool categories in rheumatic and musculoskeletal disease care
| Category | Type | Key examples | Primary functions | Clinical applications in RMD |
| Telemedicine platforms | Patient-facing | Amwell, Teladoc, Doxy.me | Remote consultations, e-consults | Follow-up, flare management, remote MDT care |
| mHealth applications | Patient-facing | RheumaBuddy, MyRA and ArthritisPower | Symptom tracking and medication reminders | RA symptom monitoring and patient education |
| Wearables and RPM | Patient-facing | Fitbit, Apple watch and weaRAble-PRO | Step count, HR, sleep and activity classification | Fatigue monitoring, rehab and flare prediction |
| DTx | Patient-facing | Kaia Health, Happify and reclarit | Software-based CBT, exercise and mindfulness | Chronic pain and fibromyalgia |
| Patient portals | Hybrid | MyChart, and Epic Portal | Test results, secure messaging and appointments | Medication adherence and patient empowerment |
| Online symptom checkers and assistants | Patient-facing | Ada Health, Buoy Health and HealthTap | AI triage and symptom guidance | Early symptom recognition |
| Medical imaging tools | Clinician-facing | Zebra Medical, Aidoc and Enlitic | Image interpretation via AI | MRI/US in arthritis diagnosis |
| Robotics in surgery/rehabilitation | Clinician-facing | MAKO and exoskeletons | Surgical precision and post-operative rehabilitation | Joint replacement and musculoskeletal recovery |
| AR/VR | Patient/clinician | Oculus VR and HoloLens AR | Pain distraction, education and rehabilitation | osteoarthritis rehab, procedure preparation |
| Wellness behaviour modification tools | Patient-facing | Headspace, Calm and Noom | Meditation, weight loss and sleep optimization | Stress reduction and comorbidity management |
| Precision medicine tools | Clinician-facing | EHR-based AI models and CDSS | Risk prediction and personalized treatment | DMARD selection and flare forecasting |
| Drug discovery tools | Research-focused | BenevolentAI and Atomwise | Target identification and drug repurposing | Novel biologics and JAK inhibitors |
| Genomics/bioinformatics tools | Clinician/research | HLA typing AI and ML for transcriptomics | Risk prediction and stratification | RA susceptibility and SLE prognosis |
AI = artificial intelligence; AR = augmented reality; CBT = cognitive-behavioural therapy; CDSS = clinical decision support systems; DMARD = disease-modifying antirheumatic drug; DTx = digital therapeutics; EHR = electronic health record; HLA = human leukocyte antigen; HR = heart rate; JAK = Janus kinase; MAKO = MAKO robotic-arm assisted surgery system; MDT = multi-disciplinary team; mHealth = mobile health; ML = machine learning; MRI = magnetic resonance imaging; RA = rheumatoid arthritis; RMD = rheumatic and musculoskeletal diseases; RPM = remote patient monitoring; SLE = systemic lupus erythematosus; US = ultrasound; VR = virtual reality.
Table 2: Summary of evidence for clinical impact of digital tools in rheumatic and musculoskeletal diseases1,3,5,10–12
| Tool type | Evidence source | Population/scope | Key outcome(s) | Effect size/impact | Reference |
| mHealth apps | Valentijn et al. (2022) | 56 RCTs; patients with MSK (including RMDs) | Pain, function and self-management | Pain SMD 0.19; Function SMD 0.14; Self-management SMD 0.14 | 1 |
| Wearables + ML | Creagh et al. (2024) – weaRAble PRO | 30 patients with RA using Apple Watch + smartphones | Continuous monitoring; RA activity classification | F1-score 0.81 for RA detection; F1-score 0.83 for severity classification | 3 |
| Digital therapeutics | Betz et al. (2024) – reclarit | Patients with RA having psychosocial burden | Anxiety, depression, fatigue, pain perception and mental health | Significant improvements in psychosocial and pain-related measures versus control | 10 |
| AI in RA management | Vlad et al. (2025) | 205 respondents (rheumatologists, GPs and patients with RA) | Early diagnosis, personalized treatment, monitoring and acceptance | Higher acceptance with prior AI exposure; barriers = cost (36%), training (37%), privacy (21%) and interoperability (42%) | 12 |
| Telemedicine | El Aoufy et al. (2024); Scoping article | 62 studies on adult patients with RMD (1990–2022) | Pain, disease activity, uric acid, mental/physical function and PROs | Increasing evidence of benefit, heterogeneous tools, telerehabilitation and tight control models promising, and guidelines needed | 5 |
| Digital rehab (VR) | Chaplin et al. (2023) | Scoping review of 51 studies on MSK rehab | Pain reduction, functional recovery and participation/adherence | Trend toward better global perceived effect versus traditional rehab; personalization and improved adherence noted | 11 |
AI = artificial intelligence; GP = general practitioner; mHealth = mobile health; ML = machine learning; MSK = musculoskeletal; PROs = patient-reported outcomes; RA = rheumatoid arthritis; RCT = randomized controlled trial; RMD = rheumatic and musculoskeletal disease; SMD = standardized mean difference; VR = virtual reality.
Figure 2: Clinical impact of digital tools in patients with rheumatic and musculoskeletal diseases
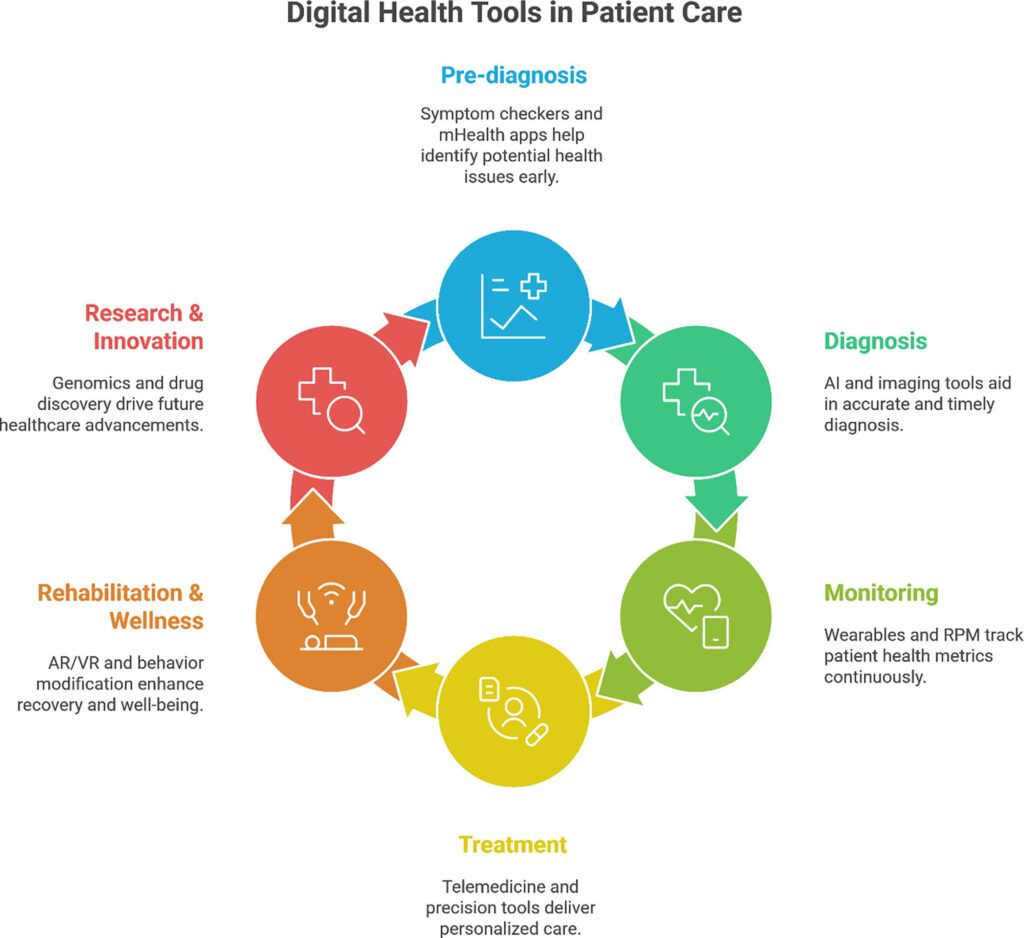
Figure 2 was created using Napkin AI (Napkin AI Inc., San Francisco, CA, USA) and Microsoft PowerPoint (Microsoft Corporation, Redmond, WA, USA). AI assistance was used solely for figure layout and visual presentation; all scientific content was conceptualized and verified by the authors.
AI = artificial intelligence; AR = augmented reality; mHealth = mobile health; RPM = remote patient monitoring; VR = virtual reality.
Telehealth and telemedicine platforms
Telemedicine delivers synchronous (video and phone) and asynchronous (e-consulting and messaging) care, which are especially crucial for rural and mobility-limited patients with RMD.5,6 Specific guidelines are available for use in patients with rheumatological diseases.15 According to a recent systematic review in rheumatology, 62 studies including 18 using mobile apps and five video consultation trials demonstrated improved pain, disease activity and patient-reported outcomes driven by telehealth interventions.4,5,13 An academic review highlights telehealth’s capacity to optimize resource use and care access but notes the need for stronger evidence and standardized guidelines.2,5 Key barriers include regulatory heterogeneity, reimbursement issues, digital literacy gaps and patient privacy concerns.5
Synchronous approaches, such as routine monthly video check-ins, have been shown to support symptom monitoring and facilitate treat-to-target strategies.4,16 Asynchronous tools, such as web-based rheumatoid arthritis (RA) activity trackers, allow patients to report symptoms and receive clinician feedback without needing scheduled appointments.3,4 Despite its advantages, telemedicine faces several implementation barriers. These include inconsistent broadband access, especially in underserved regions; the absence of standardized workflows and protocols; and ongoing concerns regarding patient data security, privacy and digital literacy.5,17 Additionally, regulatory inconsistencies and variable reimbursement policies continue to hinder widespread integration into routine rheumatologic care.2,9
Mobile health applications
Smartphone apps, as per WHO, encompass tools for health and public health supported by mobile devices. They enable symptom tracking, medication reminders and activity monitoring.3,13
A 2022 scoping review found that asynchronous mobile health (mHealth) tools for RA (e.g. gait tracking apps and remote disease activity monitors) lowered wait times and tailored care but remain underutilized.3,14,18 A systematic review on musculoskeletal digital interventions found small but significant improvements in pain (standardized mean difference [SMD] 0.19), disability (SMD 0.14) and self-management (SMD 0.14).1 However, the benefit of their utilization over the standard of care has not been fully proven.19 Thus, there needs to be a financial analysis demonstrating the benefits of their use in real life.
Popular mHealth apps such as RheumaBuddy, Rheumahelper, MyRA, and ArthritisPower offer user-friendly dashboards for tracking disease activity and enable data sharing with clinicians.3,14,20 Applications that incorporate guided exercises and medication reminders have also shown potential to improve adherence.10,20 However, challenges persist, including low long-term user engagement and the need for better clinical validation and integration with electronic health records (EHRs) and telehealth systems to optimize their clinical utility.1,20,21 There appears to be fatigue and usage declines over time.
Wearable devices and remote patient monitoring systems
Wearables [Fitbit (Google LLC, Mountain View, CA, USA) and Apple Watch (Apple Inc., Cupertino, CA, USA)] combined with remote patient monitoring (RPM) systems enable continuous physiological data capture (steps, heart rate [HR], sleep and gait) that can augment disease management.18,22 A 14-day observational study (weaRAble PRO) using smartphones + Apple Watch achieved high-accuracy classification of RA status and severity through machine learning (ML) algorithms.4,18
AI-powered systems can detect early flares and drive RPM alerts, supporting clinician interventions before symptom escalation.22
AI architectures deployed on edge or cloud platforms can classify activity and vital signs; however, challenges remain in data quality, integration and obtaining patient consent.17,22 A schematic representation of the integration of wearable-derived data with EHRs to support longitudinal RA management is shown in Figure 3.
Figure 3: Integration of wearables and electronic health records in rheumatoid arthritis management
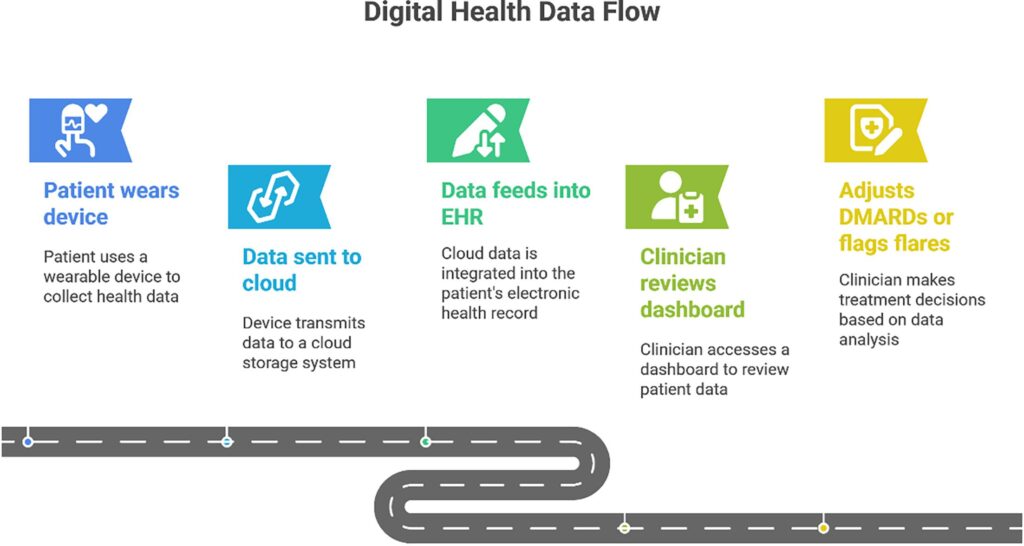
Figure 3 was created using Napkin AI (Napkin AI Inc., San Francisco, CA, USA) and Microsoft PowerPoint (Microsoft Corporation, Redmond, WA, USA). AI assistance was used solely for figure layout and visual presentation; all scientific content was conceptualized and verified by the authors.
EHR = electronic health record; DMARD = disease-modifying antirheumatic drugs.
Digital therapeutics
Digital therapeutics (DTx) are evidence-based, regulatory-approved software interventions designed to prevent or manage chronic conditions.10,20 Platforms like Kaia Health and Happify deliver guided exercise and cognitive-behavioral therapy (CBT), targeting chronic pain, fibromyalgia and similar disorders.10 Notably, reclarit, a CBT-based DTx, has shown statistically significant improvements in psychosocial outcomes among patients with RA in randomized trials.10 DTx function as adjunct treatments, typically delivered via apps or patient portals under clinician supervision.10 However, widespread adoption is limited by regulatory variation across regions and inconsistent insurance reimbursement.10,20 Similar online platforms can enable rheumatology training to far-flung areas.23,24
Patient portals
Secure, EHR-integrated portals allow patients access to lab results, medication lists, appointment scheduling and messaging tools.4,21 Benefits include improved transparency and reduced administrative workload. However, some users face accessibility barriers due to low digital literacy or limited internet access.2,4
Online symptom checkers and virtual health assistants
Tools like Ada Health and Buoy Health use AI-powered triage algorithms.3,25 Though not substitutes for medical consultation, they demonstrate high sensitivity in identifying urgent symptoms.3,25 Conversational agents (chatbots) offer 24/7 support and follow-up guidance, particularly valuable in symptom recognition and medication adherence.3,25
Medical imaging and diagnostics tools
AI-enhanced imaging tools by Zebra Medical, Aidoc and Enlitic aid interpretation of X-ray, MRI and ultrasound in arthritis, automating erosion scoring and synovitis detection.26–29 They standardize reading across radiologists and speed workflow.26,28 Tele-radiology, a subset of telemedicine, supports remote image review and reporting, leveraging broadband and secure Digital Imaging and Communications in Medicine (DICOM) standards.26,28
Robotics in healthcare
Robotic surgical systems (e.g. MAKO robotic-arm assisted surgery system (Stryker Corporation, Kalamazoo, MI, USA) and robot-assisted total knee replacement) deliver precision alignment and minimize tissue trauma in joint replacements.30 Rehabilitation robots and exoskeletons support structured recovery in physiotherapy programs.30 The field remains emergent, with promising early outcomes in RMD post-operative recovery, but larger comparative trials are needed.30
Augmented reality and virtual reality
Augmented reality (AR) and virtual reality (VR) are emerging tools in musculoskeletal care.11,31,32 AR enhances surgical accuracy by guiding intraoperative navigation in orthopedic procedures.31 VR is used for pain distraction through immersive environments, improving comfort during procedures.11 It also supports rehabilitation with gamified exercises that boost adherence and serves as an educational aid by visualizing anatomy to enhance patient understanding. A systematic review in osteoarthritis found that VR-enabled rehabilitation yielded improved pain and function.11 VR for knee and hip surgery also demonstrates benefit.31,32
Health and wellness behavior modification tools
Applications such as Noom, Headspace and Calm drive change in diet, physical activity and mindfulness, which are vital lifestyle factors in RMDs.2,25 These platforms use AI for personalized nudging and feedback. Long-term adoption remains constrained by user motivation.25
Personalized and precision medicine tools
AI-integrated CDSS extract patient data to personalize treatment, e.g. selecting disease-modifying antirheumatic drugs (DMARDs) based on phenotype and predicted response or toxicity. Predictive algorithms flag methotrexate toxicity or inadequate response using demographic, lab and patient-reported outcomes.
Emerging AI models in RA show strong predictive ability for flares and progression risk using time-series data and patient-reported outcomes.3,22
Drug discovery and development tools
AI platforms (BenevolentAI and Atomwise) are used to identify molecular targets and repurpose existing drugs for RMDs.17 These methods shorten discovery timelines and reduce cost, with case studies in Janus kinase (JAK) inhibitors and other candidate agents showing promise.17
Genomics and bioinformatics tools
AI-driven genomics enables large-scale analysis of human leukocyte antigen (HLA) alleles (e.g. RA risk), integrates transcriptomics/proteomics for patient stratification and identifies biomarkers in diseases such as systemic lupus erythematosus (SLE) and scleroderma. These tools underpin personalized therapy and prognosis.3,17,22
Management tools for digital health
An equally important but often under-recognized dimension of digital health is data and operations management software. These can be studied under seven domains.
Electronic health records/electronic medical records
EEHRs represent digital counterparts of traditional paper-based patient records. In rheumatology, EHR systems play a critical role in monitoring chronic conditions such as RA, SLE and ankylosing spondylitis (AS).1,4 These systems store comprehensive clinical information, including patient symptoms, laboratory results, prescribed medications and disease activity indices such as Disease Activity Score 28 (DAS28), Ankylosing Spondylitis Disease Activity Score (ASDAS) and Bath Ankylosing Spondylitis Disease Activity Index (BASDAI), which are essential for assessing disease progression and treatment response.4,13
In high-income countries such as the United States, EHR implementation is widespread. An analysis of electronic medical record (EMR) data from 5,900 RA patients demonstrated that AI algorithms could accurately predict disease activity from clinical documentation, achieving a positive predictive value of 0.94.3,22 Furthermore, EHR systems in the USA are often integrated with specialty registries such as the American College of Rheumatology’s RISE registry, facilitating real-time data analysis, benchmarking and quality improvement.3,4
In contrast, EHR adoption in India is expanding gradually but remains primarily confined to tertiary-care centers and urban specialty clinics.5 Many small and medium-sized practices continue to rely heavily on paper-based documentation. A 2022 publication in the Indian Journal of Rheumatology highlighted the need for rheumatology-specific EHR templates aligned with national data standards.5 A subsequent 2025 study evaluating open-source EHR platforms reported that OpenEMR satisfied approximately 74% of the Government of India’s minimum data requirements, identifying it as a promising candidate for broader implementation.5,9 Persistent challenges include high deployment costs, shortages of trained personnel, inadequate digital infrastructure in rural regions and resistance to transitioning from paper-based to electronic systems.5,9
Health information exchange and interoperability solutions
Health information exchange (HIE) systems enable hospitals, clinics and laboratories to securely share patient data across institutions, thereby supporting continuity of care.2,9 This function is particularly vital for rheumatology patients, who often require multidisciplinary management involving multiple specialists.2,4
In high-income countries, HIE systems are commonly based on interoperability standards such as Health Level Seven Fast Healthcare Interoperability Resources (HL7 FHIR), which facilitate seamless communication between EHRs and digital health applications. Nevertheless, achieving full interoperability remains challenging even in advanced healthcare systems. For example, hospitals within the United Kingdom’s National Health Service often encounter difficulties in exchanging data across different administrative trusts due to variations in IT infrastructure and data governance protocols.2
In India, the Ayushman Bharat Digital Mission (ABDM), launched in 2021, aims to establish a nationwide interoperable digital health ecosystem. The initiative encompasses several key components, including the Ayushman Bharat Health Account (ABHA) providing a unique health identifier, national registries for healthcare professionals and facilities, mechanisms for linking and sharing patient health records and the Health Claim Exchange (HCX) for streamlined and paperless insurance processing. As of early 2025, more than 760 million ABHA IDs had been generated, and approximately 520 million health records were digitally linked under the ABDM framework.5,9 In addition, over 800 digital health applications and platforms had been integrated with the ecosystem. Despite these significant advances, persistent challenges such as limited digital literacy, inadequate infrastructure in rural regions and varying levels of technological readiness continue to impede the widespread adoption and effective utilization of HIE in India.5,9
Healthcare customer relationship management systems
Customer relationship management (CRM) systems are digital platforms designed to manage and optimize patient relationships across the continuum of care. These systems support appointment scheduling, medication reminders, follow-up tracking and personalized communication, including health education messages and notifications about laboratory results.2,25 Although direct evidence in rheumatology is limited, CRM solutions in broader healthcare settings have been associated with improved patient satisfaction, reductions in missed appointments and better adherence to treatment plans.25
In rheumatology, CRM tools can facilitate treat-to-target strategies by generating automated notifications for clinicians and patients when follow-up visits or laboratory monitoring are due. These alerts can be linked to disease activity assessment instruments, such as the Health Assessment Questionnaire and Disease Activity Score 28 (DAS28), thereby supporting systematic monitoring and timely therapeutic adjustments.4,16
In the Indian context, mobile-based reminder systems using short message service (SMS) or applications such as WhatsApp are increasingly used, particularly in urban settings, to support patient engagement and adherence in chronic diseases. Such low-cost, widely accessible tools can help overcome barriers related to distance, limited health awareness and irregular follow-up, thereby enhancing continuity of care and adherence to long-term rheumatologic therapies.5,25
Business process management systems
Business process management (BPM) systems map, standardize and automate clinical workflows, such as patient registration, check-in, laboratory ordering, prescription processing and insurance claims handling. By formalizing these processes, BPM tools enhance consistency, reduce manual errors and support more efficient care delivery in complex clinical environments.2,9
Although evidence specifically focused on rheumatology is limited, BPM methodologies have been successfully applied in healthcare systems in high-income countries to improve care coordination and streamline both clinical and administrative pathways. In Europe, hybrid rheumatology care models that combine in-person and virtual visits have used BPM-based platforms to manage follow-up scheduling, electronic patient-reported outcomes and digital communication, demonstrating the feasibility of structured, process-driven care delivery.2,30
In India, BPM solutions are being progressively implemented in large corporate hospitals and multispecialty institutions, often as part of broader workflow automation or hospital information system initiatives. However, most rheumatologists practice in smaller clinics that typically lack formalized workflows and rely on manual processes. Digitizing repetitive tasks such as registration, follow-up appointment scheduling and retrieval of laboratory reports through BPM could substantially reduce administrative burden, save time and improve the quality and continuity of rheumatology care in these settings.5,9
Enterprise content management
Enterprise content management (ECM) in healthcare refers to integrated methods, tools and processes used to manage digital information across an organization.2,9 It encompasses the systematic organization, storage and retrieval of clinical content such as laboratory reports, radiology images, discharge summaries and referral documents.2 By consolidating this information, ECM enhances information flow between healthcare providers and accelerates access to patients’ longitudinal records.9
In rheumatology, where patients frequently undergo repeated imaging and serial laboratory assessments over many years, ECM helps ensure that all relevant documents are centrally archived and readily accessible at the point of care.9,29 Such systems also support teleconsultations and telemedicine services by enabling secure remote access to the same clinical content, maintaining continuity and quality of care in virtual settings. In India, large urban hospitals and corporate healthcare networks have begun implementing ECM solutions, often integrated with EHR or hospital information systems, to manage high volumes of clinical and administrative documents.5 However, many smaller clinics still depend on paper files or fragmented digital storage, contributing to incomplete documentation, delays in diagnosis and potentially avoidable repeat testing that increase both costs and patient burden. By streamlining document-intensive workflows and reducing reliance on paper-based systems, ECM can lower operational costs, improve record reliability and support more efficient, patient-centered care.5,9
Cybersecurity and data protection solutions
As digital health systems proliferate, safeguarding patient data through robust cybersecurity measures becomes paramount.2,9 Essential tools include data encryption, multi-factor authentication, role-based access controls and secure cloud storage solutions.22 High-income countries enforce stringent regulations such as the Health Insurance Portability and Accountability Act (HIPAA) in the USA and the General Data Protection Regulation (GDPR) in Europe, which govern the storage, access and sharing of patient information.2
In India, the Digital Personal Data Protection Act, 2023, mandates explicit, informed patient consent for data processing and establishes guidelines for secure data management. The ABDM incorporates security features such as token-based authentication, audit logs and user verification to protect health records.5,9 Nevertheless, data breaches and privacy lapses persist despite these frameworks. This underscores the critical need for rigorous enforcement of regulations, enhanced public awareness campaigns and comprehensive training programs for healthcare providers on data privacy best practices.2,9
Medical coding and billing software
Medical coding systems translate clinical diagnoses into standardized alphanumeric codes, such as those from the International Classification of Diseases, Tenth Revision, facilitating accurate billing, insurance claims processing and epidemiological analysis. Billing software leverages these codes to generate invoices, submit claims electronically and stratify patients into disease-specific cohorts, which support research initiatives such as outcome studies and cohort matching.9
In high-income healthcare settings, this process is fully automated and seamlessly integrated with EHRs, enabling rheumatologists to efficiently code conditions such as RA (e.g. M05), SLE (M32) and gout (M10).4,9 In India, manual billing predominates in many rheumatology practices, leading to inefficiencies, errors and delays in reimbursement. The introduction of the HCX under the ABDM is transforming this landscape by enabling real-time digital submission, verification, adjudication and approval of insurance claims, thereby minimizing paperwork and processing times.5,9 HCX standardizes interoperability across payers, hospitals and third-party administrators, promoting cashless transactions even for out-patient services. As more rheumatology clinics participate in health insurance programs, automating medical coding and billing will become essential to reduce administrative burdens, enhance revenue cycle management and support scalable participation in medi-claim schemes.5,9
Evidence synthesis: efficacy and clinical impact
Digital health tools have shown modest but significant benefits in managing RMDs.1,22 A meta-analysis of 56 randomized controlled trials (RCTs) found that mobile apps and telerehabilitation lead to small improvements in pain and function (SMD 0.14–14–0.24).1,13,14 Evidence is strongest for back pain rehabilitation, with moderate support for shoulder and hip interventions.11,31,32 Digital therapeutics like reclarit have improved anxiety and depression in RA patients, while symptom-tracking apps correlate with reduced disease activity.10 AI-based imaging enhances diagnostic consistency, though effect sizes are still emerging. Remote care can reduce healthcare utilization, but more economic evaluations and equity-focused strategies are needed, especially for low-resource settings.2,9,25 The overall clinical impact of digital interventions across pain, function, mental health and disease activity outcomes is summarized in Figure 2.
Ethical, regulatory and implementation considerations
Widespread digital health adoption raises ethical and regulatory concerns, particularly around data privacy and compliance with standards like GDPR and HIPAA.2 The digital divide especially affects older adults, rural populations and low-income groups, limiting both access and effectiveness.5,9 AI tools also risk algorithmic bias if not validated across diverse populations.17,26,27 Many apps lack formal clinical validation or regulatory approval, and integration into workflows remains limited.21 Clinician involvement in design is crucial to ensure adoption and effectiveness.4,25 The key challenges and enabling opportunities influencing the adoption of digital health tools in rheumatology are summarized in Figure 4.
Figure 4: Challenges and opportunities in digital health implementation in rheumatology
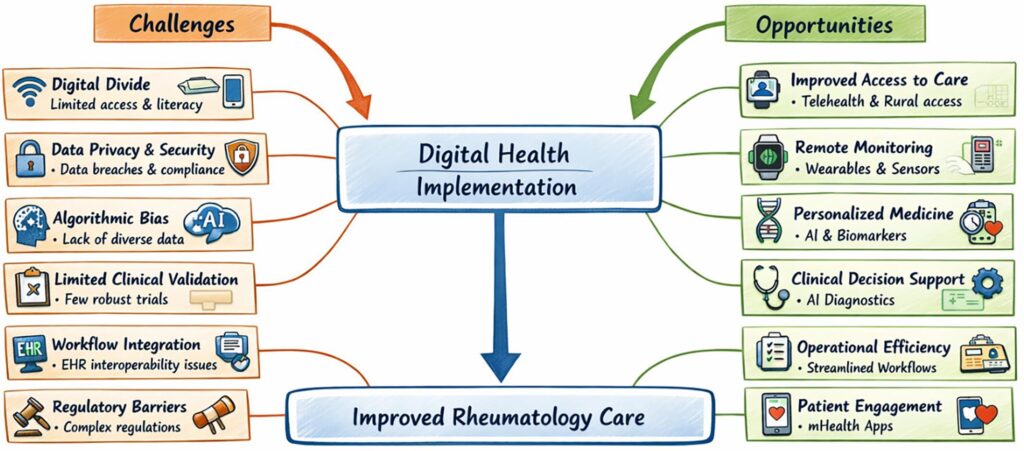
Figure 4 was created using ChatGPT (OpenAI, San Francisco, CA, USA) and Microsoft PowerPoint (Microsoft Corporation, Redmond, WA, USA). AI assistance was used solely for figure layout and visual presentation; all scientific content was conceptualized and verified by the authors.
AI = artificial intelligence; EHR = electronic health record; mHealth = mobile health.
Future directions
To fully harness the potential of digital health tools in rheumatology, several strategic priorities must be addressed. First, there is a critical need for high-quality, adequately powered randomized controlled trials that evaluate both clinical and economic outcomes across varied care settings.1,13,14,20 Hybrid care models, which combine in-person and digital approaches such as RPM-enabled treat-to-target strategies, may offer enhanced flexibility and responsiveness.10,18,22
Equally important is the development of standardized frameworks for data integration, clinical outcome measurement and interoperability across platforms and health systems.4,5,9 Patient-centered co-design will play a pivotal role in improving usability and adoption; involving patients in the design and feedback stages ensures that tools align with real-world needs and preferences.3,20 On the regulatory front, innovative pathways are required to streamline the approval, reimbursement and scaling of digital therapeutics and AI algorithms.2,10,17
Lastly, efforts must be made to design and implement scalable solutions suitable for low- and middle-income countries, with an emphasis on accessibility, affordability and infrastructure development to bridge the global digital divide.5,9
Conclusion
Digital health tools, particularly those powered by AI, are reshaping diagnostics, monitoring, therapy, behavior change and research in RMD care. Evidence shows consistent though modest clinical benefits and strong potential for personalized, remote and patient-centered care.1,10,13,20 Addressing validation, equity and clinical integration hurdles through collaboration, rigorous research and policy innovation will be crucial to harness their full potential.2,5,9,17
On the operational front, digital health tools have proven helpful in prioritizing sicker patients, supporting triage and optimizing pathways to minimize wastage of healthcare resources.4,9,22 With structured implementation, ethical oversight and patient engagement, these tools could transform RMD management globally, enabling more efficient, equitable and personalized care.1–3,5,9











